Principles of Peeling Procedures Explained by a Dermatologist and Suitable Candidates for Each of the 3 Types
Peeling is a chemical reaction that controls penetration depth through pH and concentration. Epidermal (AHA), porous (BHA), and dermal (TCA) types differ in their layers of action. Even with the same glycolic acid, there is a three-fold difference in recovery time between a 30% pH of 2.8 and a 70% pH of 1.5. The pH setting determines the results more than the concentration. For oily skin in your 20s and pigmented skin in your 40s, peeling agents…
The Science of Chemical Exfoliation
- Operates in the pH range of 0.5 to 3.5
- Adjusts depth from epidermis to 0.6 mm
- 12 FDA-approved ingredients
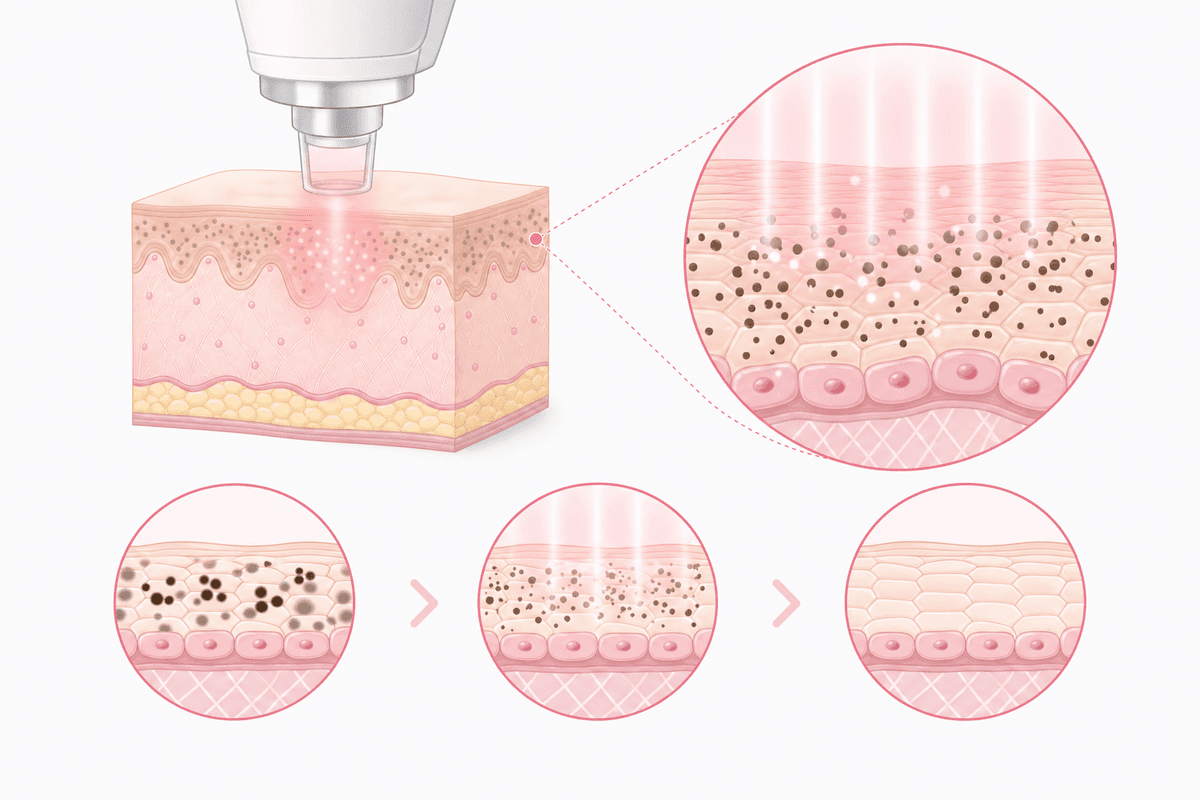
Peeling does not ‘strip away’ but ‘breaks protein bonds’
“Isn’t it just removing dead skin cells?” — This question causes 90% of people to misunderstand peeling. Peeling is a procedure that chemically breaks down desmosome proteins responsible for adhesion between keratinocytes.
When an acidic solution with a pH of 3.0 or lower comes into contact with the skin, the calcium ion bonds between keratinocytes are broken. During this process, the stratum corneum loosens and shedding begins. Since the FDA approved a 70% concentration of glycolic acid in the 1990s, 12 types of peeling agents with a pH range of 0.9 to 3.8 are currently used in clinical practice. Even with the same ingredients, a difference of 0.5 in pH results in a penetration depth of 0.1 mm. The epidermal thickness averages 0.1 mm, and the depth to the upper dermis is 0.6 mm. Peeling is a procedure that targets this range by adjusting the concentration and pH to design 'to which layer the proteins will be released.' According to a 2021 report by the Korean Dermatological Association, the rate of skin regeneration after peeling is proportional to the penetration depth. The epidermal type undergoes a turnover cycle of 3–5 days, while the dermal type undergoes 7–14 days.
- Desmosome protein degradation → Shedding of the stratum corneum
- Calcium bond breaking at pH 3.0 or below
- 12 FDA-approved peeling agents, pH range 0.9–3.8
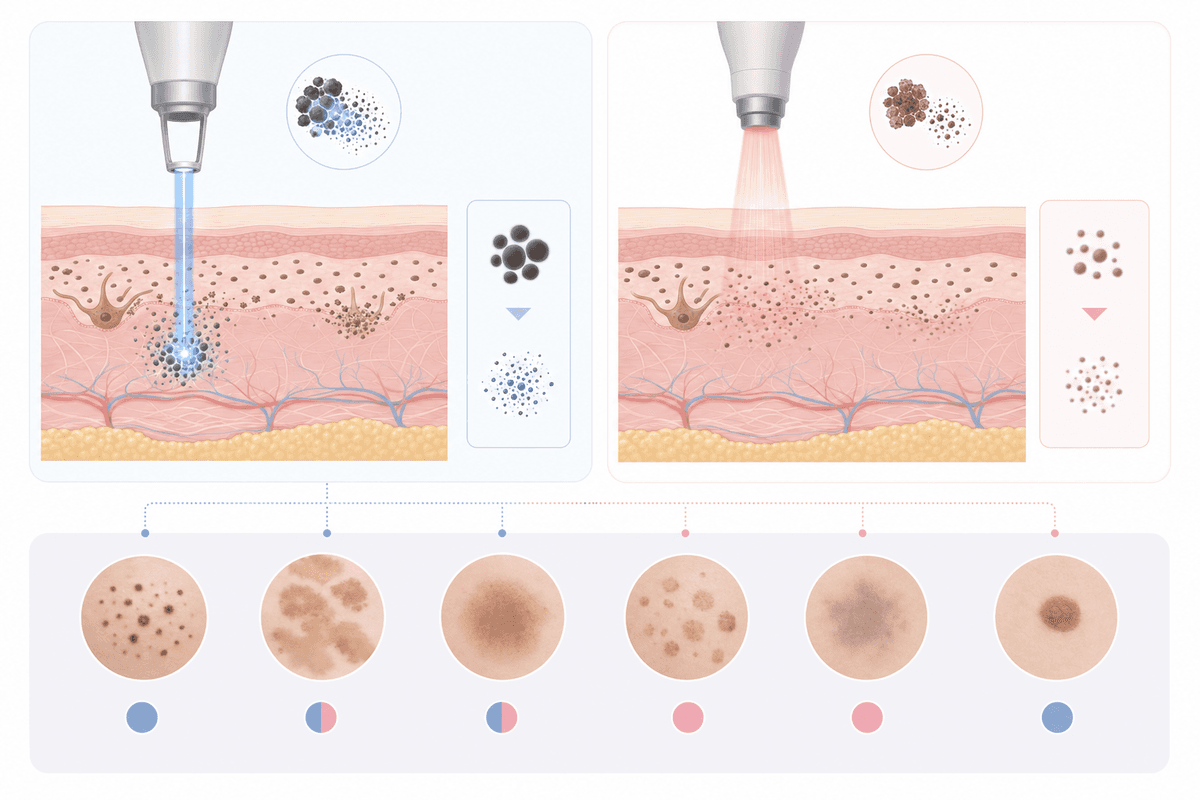
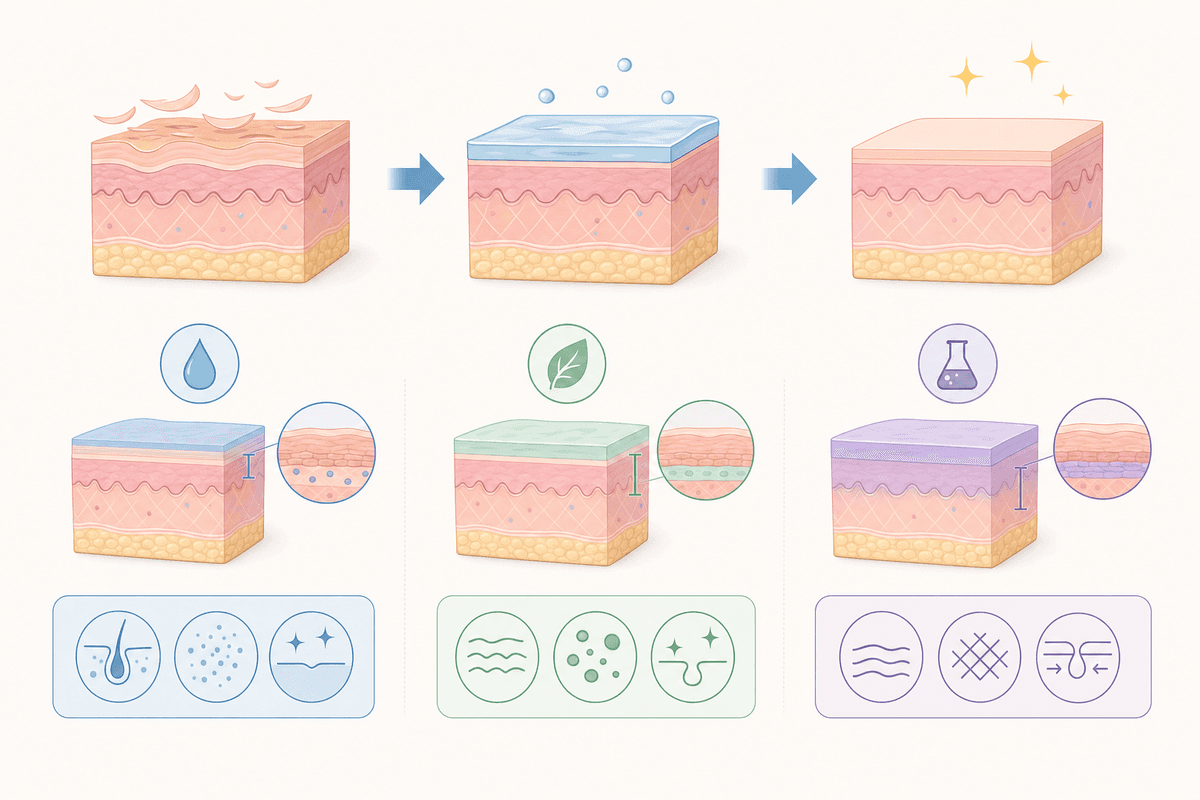
Epidermal type (AHA) vs. Pore type (BHA) — Solubility determines the target
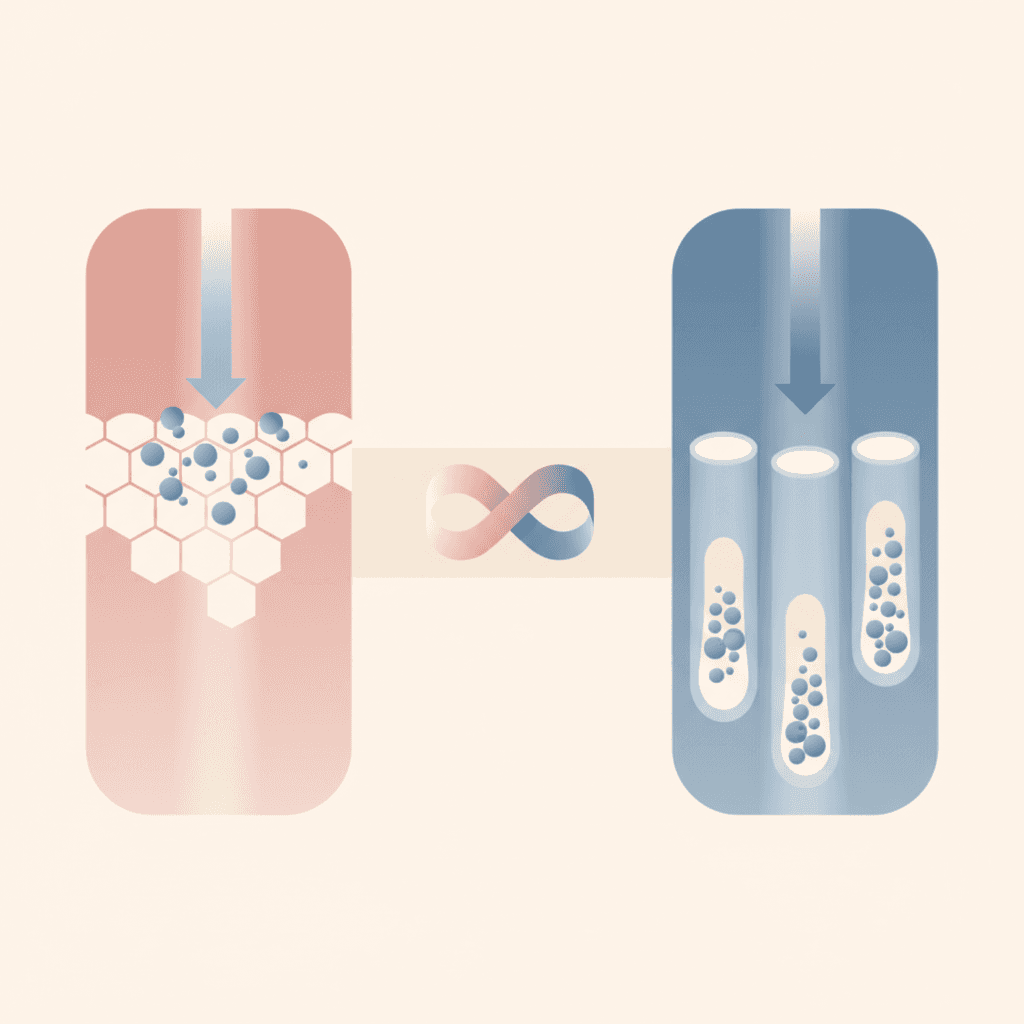
Peeling agents are broadly divided into water-soluble AHA (Alpha Hydroxy Acid) and fat-soluble BHA (Beta Hydroxy Acid). This difference makes the results after the procedure completely different. Glycolic Acid and Lactic Acid, the representative ingredients of AHA, dissolve in water and rapidly penetrate the stratum corneum of the epidermis. At concentrations ranging from 30% to 70%, they evenly exfoliate the entire epidermis (0.1–0.15 mm). On the other hand, Salicylic Acid in BHA dissolves in sebum and penetrates deep into the pores. Even at concentrations of 20–30%, it reaches the opening of the sebaceous gland (0.2 mm deep) to remove comedonal acne and blackheads. In clinical practice, Glycolic Acid 50% pH 2.5 is the primary choice for improving pigmentation, while Salicylic Acid 20% pH 3.0 is the primary choice for acne-prone skin. Even though they are the same 'peeling', their mechanisms of action differ. Key Point: If you use AHA on oily skin, only the surface is peeled, leaving sebum inside the pores. If you use BHA on dry skin, the dryness worsens due to excessive oil removal. Selecting the right solubility is half the success of the procedure.
| Ingredients | Solubility | Penetration Depth | Main Targets |
|---|---|---|---|
| Glycolic Acid | Water-soluble | Epidermis 0.1~0.15mm | Pigmentation, rough texture |
| Lactic Acid | Water-soluble | Epidermis 0.08~0.12mm | Dry, Fine wrinkles |
| Salicylic Acid | Oily | 0.2mm inside pores | Acne, sebum |
- AHA: Water-soluble, targets epidermis
- BHA: Oil-soluble, targets pores
- Difference in use between Glycolic Acid 50% vs. Salicylic Acid 20%
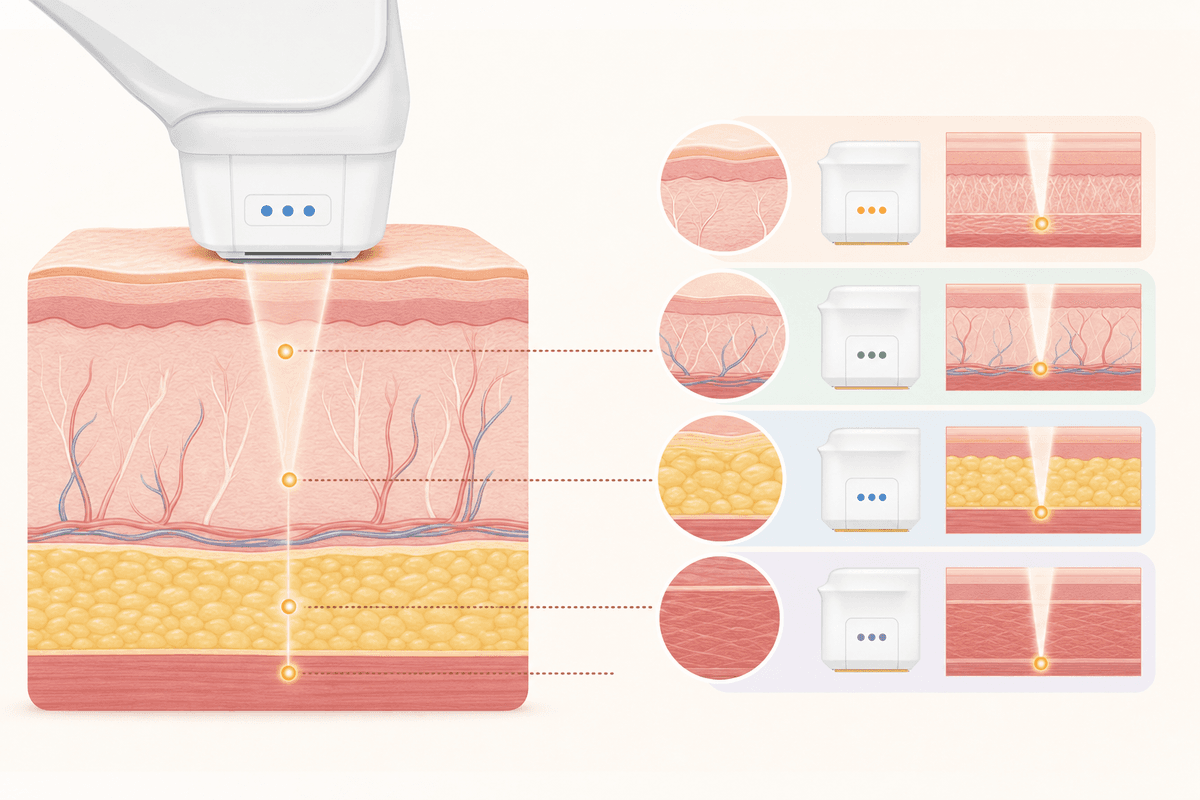
Dermal Peeling (TCA) — Touches collagen at a depth of 0.3mm
TCA (Trichloroacetic Acid) is a medium-to-high intensity peeling agent that penetrates beyond the epidermis to the upper dermis (0.3~0.6mm). It is used in a concentration range of 15–35%, and concentrations of 30% or higher are for medical institutions only. TCA induces a protein coagulation reaction. When fibroblasts in the dermis are damaged, TGF-β (Transforming Growth Factor-beta) signals are immediately secreted, and new collagen synthesis begins over a period of 7 to 10 days. According to 2020 clinical data from the Korean Academy of Aesthetic Plastic Surgery, dermal collagen density increased by an average of 18% after three treatments with 25% TCA. This is an effect not observed in epidermal peeling. However, the recovery period is long, ranging from 7 to 14 days, and immediate neutralization is required if frosting (formation of white crystals) occurs during the procedure. Excessive penetration increases the risk of scarring. Caution: TCA concentrations of 30% or higher can lead to dermal damage if depth control fails. It must be performed at a medical institution equipped with patch testing and neutralization protocols.
- TCA penetration depth 0.3~0.6mm
- Protein coagulation → TGF-β secretion → Collagen resynthesis
- 25% Collagen density +18% after 3 treatments
20s Sebaceous Type vs. 40s Pigmented Type — Criteria for selecting peeling by skin type
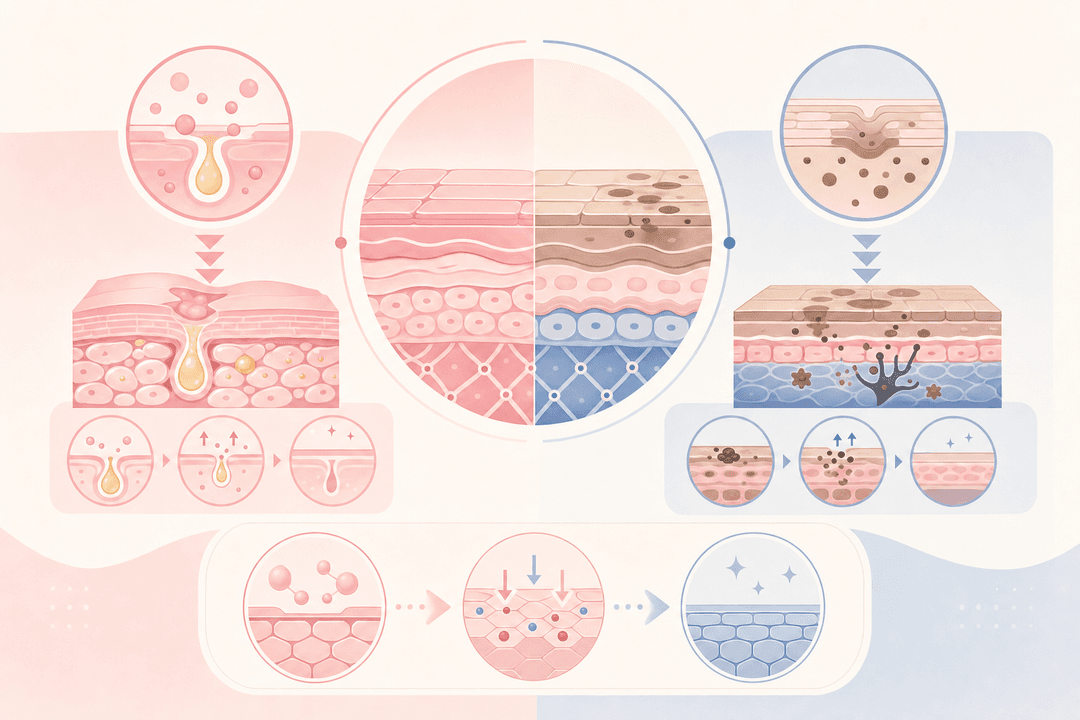
For oily and acne-prone skin in the 20s, excessive sebum secretion and keratinization of the pores are the issues. In this case, a 20–30% salicylic acid peel is the primary choice. Because it is oil-soluble, it penetrates deep into the sebaceous glands to directly dissolve comedones.
For pigmented skin in the 30s and 40s, melanin granules are accumulated in the basal layer of the epidermis. The pigment must be exfoliated uniformly across the entire epidermis using a 50–70% glycolic acid peel with a pH of 2.5 or lower to ensure the pigment is shed along with it.
For skin with reduced elasticity in the 40s and older, dermal collagen density is decreased. In this case, it is effective to induce dermal remodeling with a medium-intensity TCA peel of 15–25%. Find a clinic at K-Dia where you can receive a skin type diagnosis and consult on suitable peeling agents. Places equipped with skin analysis equipment provide accurate pH and concentration matching. Tip: Skin type is not determined by age alone. Even in your 40s, BHA may be the priority if you have an oily skin type, while AHA is suitable for those in their 20s if they have a pigmented skin type. Combination types can also be used in combination.
| Skin Type | Key Problem | Recommended Peeling Agent | Concentration·pH |
|---|---|---|---|
| 20s Oily Skin·Acne | Excessive Sebum, Keratosis of Pores | Salicylic Acid (BHA) | 20~30%, pH 3.0 |
| 30s~40s Pigmentation | Melanin Granules Accumulation | Glycolic Acid (AHA) | 50~70%, pH 2.5 |
| 40s+ Loss of Elasticity | Decrease in Collagen Density | TCA | 15~25%, pH 1.5 |
- Oily skin → Salicylic acid 20~30%
- Pigmented skin → Glycolic acid 50~70%
- Loss of elasticity type → TCA 15~25%
Variables more important than concentration — pH and contact time determine results
Even with the same 70% Glycolic Acid, pH 1.2 and pH pH 2.8 is a completely different procedure. The lower the pH, the higher the degree of dissociation, allowing more hydrogen ions to penetrate the skin. In clinical practice, 70% glycolic acid at pH 1.5 reaches the upper dermis with 2 to 3 minutes of contact, whereas pH 2.8 remains in the middle layer of the epidermis even after 5 to 7 minutes of contact. pH control is the key to depth design. While there are products with fixed pH levels by brand, such as Obagi Blue Peel (TCA 20–30%), most medical institutions measure the pH in real-time using a pH meter and adjust the concentration accordingly. Contact time is also important. 30% salicylic acid penetrates deep into the pores within 3 minutes, but excessive dryness and erythema occur if it exceeds 5 minutes. Timer management is essential. Key Point: 70% of peeling failures stem from errors in pH settings and contact time management. Do not undergo the procedure based solely on the figure of '70% peeling'. Check the pH and time protocol.
- pH 1.2 vs 2.8 → 2x difference in penetration depth
- Glycolic acid 70% pH 1.5 = 2–3 minutes contact
- Salicylic acid 30% Risk of excessive dryness if exceeding 5 minutes
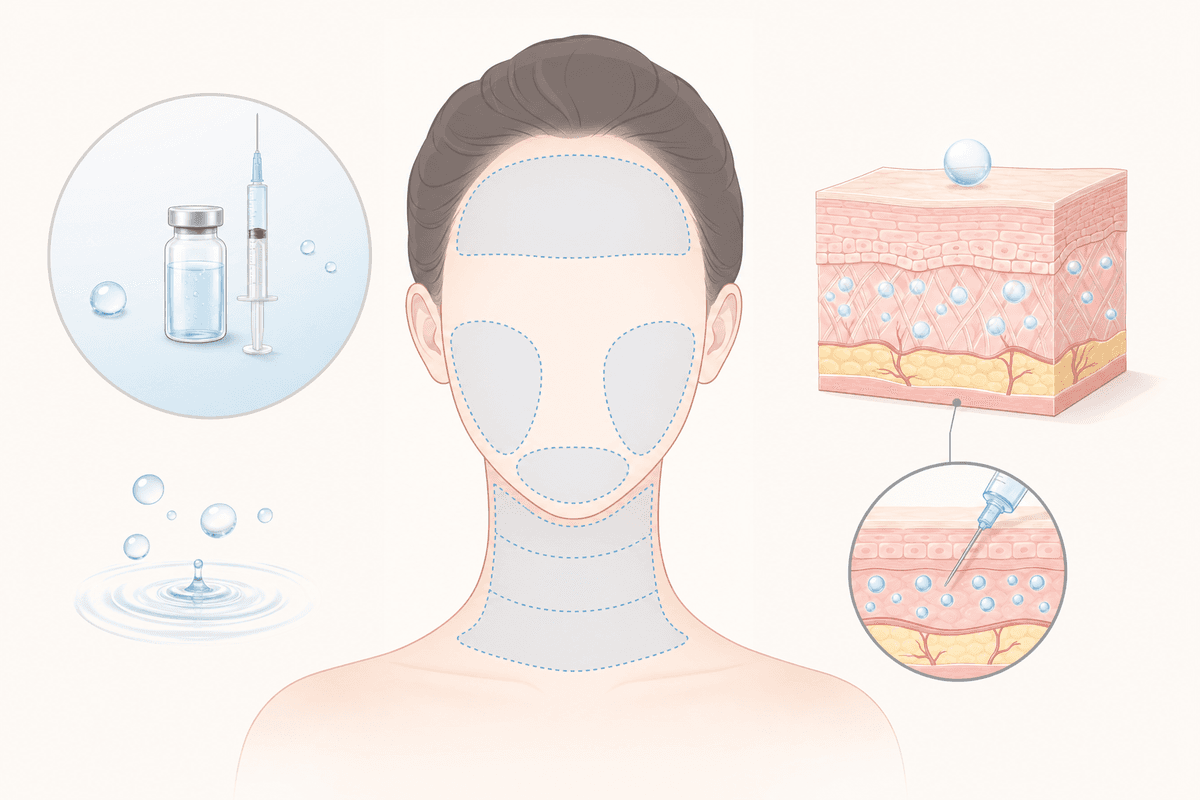
48 hours post-procedure — Neutralization and moisturization are half the result
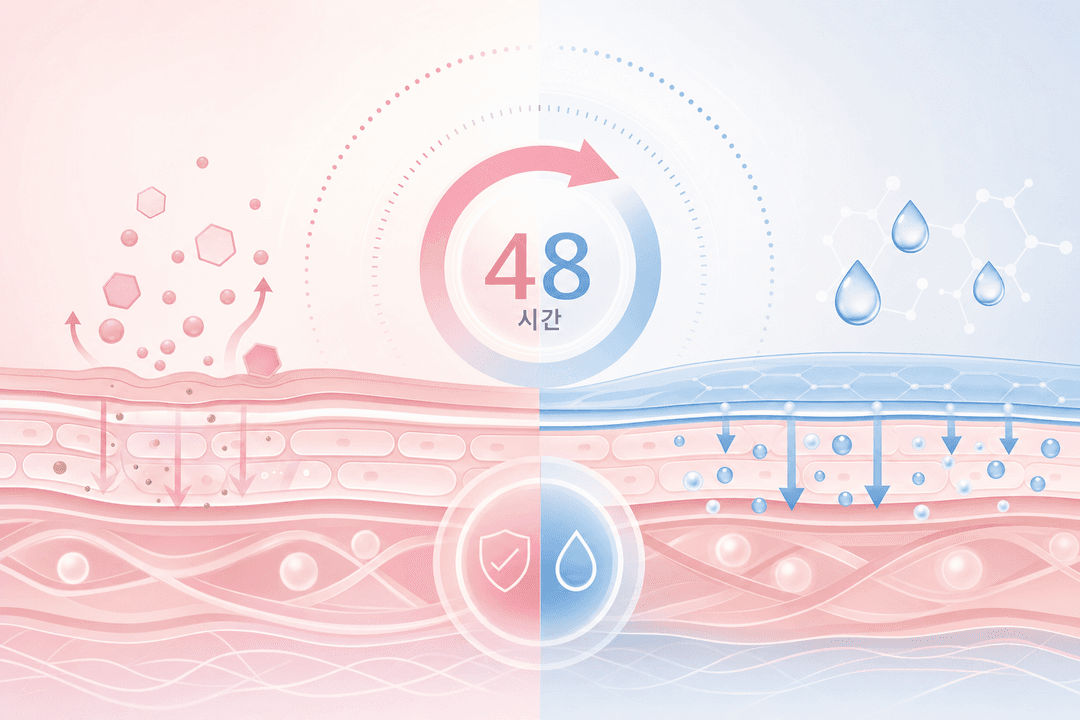
Immediately after peeling, the skin pH drops below 3.0. In this state, a neutralizing agent (such as sodium bicarbonate) must be applied immediately to stop the acidic reaction. If left untreated without neutralization, excessive exfoliation will occur.
Transepidermal water loss (TEWL) is three times higher than usual 24 to 48 hours after the procedure. Moisturizers containing hyaluronic acid or ceramide should be applied 4 to 5 times a day to reduce dryness and stinging.
Exfoliation occurs over 3 to 5 days for epidermal peels and 7 to 10 days for TCA dermal peels. Forcibly removing dead skin cells during this period increases the risk of post-inflammatory hyperpigmentation (PIH) by three times. Using a soothing cream approved by the Ministry of Food and Drug Safety (containing Panthenol, Cica, or Aloe Vera) in combination shortens the duration of erythema by an average of 40%. Check K-Dia for hospitals with strong recovery care. Caution: Sauna, alcohol consumption, and high-intensity exercise within 48 hours of the procedure worsen erythema due to vasodilation. Sunscreen (SPF 30 or higher) is essential when going outdoors.
- Immediately after treatment, pH 3.0 or lower → Neutralization essential
- TEWL increases 3-fold → Apply moisturizer 4-5 times a day
- Forced exfoliation increases PIH risk by 3 times
Comparison by Peeling Type
AHA Epidermal Peeling [Improves Pigmentation & Texture]
- Ingredients: Glycolic Acid, Lactic Acid
- Penetration: 0.1~0.15mm into the epidermis
- Recovery: 3~5 days
- Suitable: Pigmentation, rough skin
Water-soluble, so it exfoliates the entire epidermis evenly
BHA Pore Peeling [Acne & Sebum Management]
- Ingredients: Salicylic Acid
- Penetration: 0.2mm into pores
- Recovery: 3~5 days
- Suitable: Oily, acne-prone skin
Oily-soluble, so it penetrates deep into the sebaceous glands
TCA Dermal Peeling [Elasticity & Wrinkle Improvement]
- Ingredients: TCA 15~35%
- Penetration: Upper dermis 0.3~0.6mm
- Recovery: 7~14 days
- Suitable for: Loss of elasticity, deep wrinkles
Induces collagen resynthesis, for medical institutions only
Common Misconceptions
Misconception Peeling is more effective the higher the concentration
Truth pH and contact time are more important than concentration. Glycolic acid at 50% pH 1.5 for 3 minutes can penetrate deeper than at 70% pH 2.8 for 7 minutes. Setting the pH according to your skin type and goals is key to a successful peel. Unconditionally pursuing high concentrations only increases the risk of excessive exfoliation and PIH.
Misconception If dead skin cells do not peel off after a peel, the procedure is a failure.
Truth Very superficial peeling does not show dead skin cells to the naked eye. This is because it works by only loosening the bonds between keratinocytes to promote cell turnover. In fact, thick layers of dead skin peeling are a sign of a medium-intensity or higher peel. The effect should be evaluated based on skin texture and tone after 2 to 4 weeks.
Absolutely Prohibited Actions Before and After Peeling Procedure
- Stop using retinol, AHA, or BHA cosmetics 2 weeks prior to the procedure (Excessive penetration when the stratum corneum is thinned)
- Do not use makeup or cleansing foam on the day of the procedure (Surfactants interfere with the peeling agent's reaction)
- Do not use forced exfoliation, peeling packs, or scrubs within 48 hours after the procedure (3 times higher risk of PIH)
- Do not use saunas, steam rooms, alcohol, or high-intensity exercise during the recovery period (Erythema worsens due to vasodilation)
- Do not go out without sunscreen for 2 weeks after the procedure (5 times higher risk of hyperpigmentation)
Frequently Asked Questions
For epidermal peeling (AHA/BHA), you can wash your face with lukewarm water starting 24 hours after the procedure. However, we recommend using a low-irritation cleansing water instead of cleansing foam. For TCA dermal peeling, you can wash your face gently starting 48 hours later, but you should pat your face dry rather than rubbing.
I have acne-prone skin; which is right for me, AHA or BHA?
If your acne is mainly inflammatory (in the form of red bumps), a 20–30% salicylic acid (BHA) peel is suitable. Because it is oil-soluble, it penetrates deep into the sebaceous glands and directly dissolves comedones. If acne scars (hyperpigmentation) are a concern, a 50% glycolic acid (AHA) peel is more effective.
After peeling, thick layers of dead skin cells appear; can I peel them off?
Absolutely not. Forcibly removing dead skin cells before they naturally slough off increases the risk of post-inflammatory hyperpigmentation (PIH) by three times. You must apply plenty of moisturizer and wait 7 to 10 days. If the peeling is a concern, consult a medical institution for soothing care.
Which should I do first, peeling or laser treatment?
It depends on the purpose. If hyperpigmentation is the primary goal, it is effective to cleanse the epidermis with a peel and then combine it with a toning laser 4 to 6 weeks later. If the goal is to improve skin elasticity, the general procedure is to perform a laser treatment (such as fractional laser) first, and then refine the epidermis with a peel 2 to 3 weeks later. How long do the peeling effects last? The effects of epidermal peels (AHA/BHA) last for 4 to 8 weeks, while TCA dermal peels last for 3 to 6 months. However, there are significant individual differences depending on UV exposure and skin care habits. Combining regular maintenance peels (every 6 to 8 weeks) with home care (retinol/vitamin C serum) helps extend the effects. Is peeling possible during pregnancy or breastfeeding? The use of salicylic acid (BHA) is not recommended during pregnancy. On the other hand, while there are reports that glycolic acid (AHA) and lactic acid are possible at low concentrations (30% or less), individual differences exist, so you must consult with an OB/GYN or dermatologist before making a decision.
This content is for informational purposes only and does not replace medical advice. Results of peeling procedures vary significantly depending on skin type, pH, and concentration, so please be sure to consult with a specialist before proceeding. Individual differences exist, and you must visit a medical institution immediately if side effects (erythema, pigmentation, infection, etc.) occur.