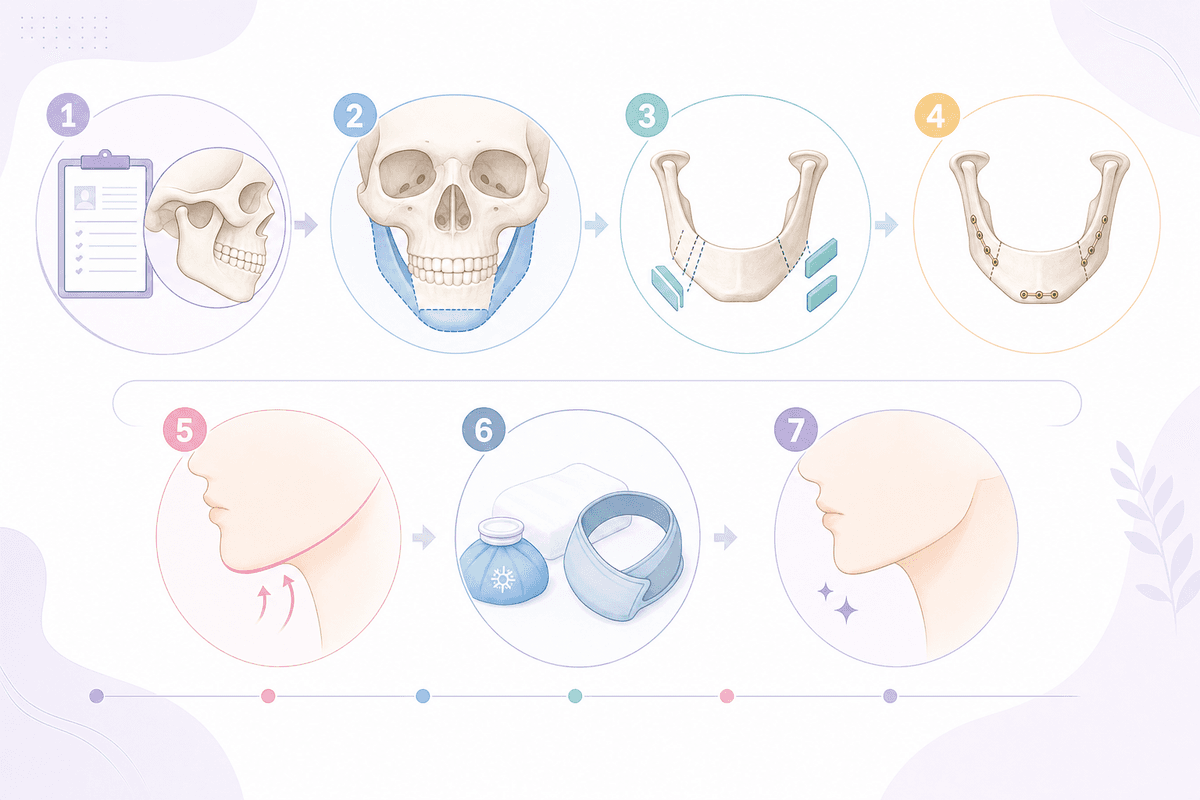
We will explain the 7-step facial contouring surgery process thoroughly, from consultation to recovery.
Contouring surgery pre-simulates osteotomy locations to 0.1mm accuracy using 3D CT-based Virtual Surgery Planning (VSP), and reduces the risk of nerve damage by 73% during surgery using Piezo Surgery equipment. The standard range is an average mandibular angle of 15-22mm for square jaw resection and an average zygomatic arch displacement of 5-8mm for cheekbone reduction, and…
Actual Surgical Process Explained by Specialists
- CT scan with a minimum slice thickness of 0.625mm
- Average general anesthesia duration: 2.5-4 hours
- Minimum 6 months for complete bone fusion
Overview at a Glance
- Contour surgeries utilize 3D CT-based Virtual Surgery Planning (VSP) to pre-simulate osteotomy positions down to 0.1mm. During surgery, Piezo Surgery equipment reduces the risk of nerve damage by 73%.
- For square jaw reduction, the standard mandibular angle resection is 15-22mm, and for cheekbone reduction, the zygomatic arch posterior repositioning is 5-8mm. Excessive resection can lead to secondary angle formation and accelerated aging.
- Post-surgery swelling in the first week increases facial volume by an average of 142% compared to pre-operative volume. Intravenous administration of 1g Tranexamic acid can reduce blood loss by an average of 38%.
Step 1: Precision Imaging — CT Protocols and Analysis
The most crucial part of contour surgery consultation is the 3D CT scan. While a standard panoramic X-ray only provides 2D information, Cone Beam CT (CBCT) captures the mandibular nerve canal, mental foramen, and zygomatic arch thickness in 3D with a slice thickness of 0.625mm. Reconstructing CT data with software like Simplant Pro or Mimics allows for 3D visualization of nerve pathways.
For patients with facial asymmetry, Frontal Cephalometry is additionally performed to quantify the midline deviation angle (average 2-5 degrees) and mandibular angle height difference (average 3-7mm). This data serves as the basis for determining the osteotomy amount during surgery, with a target symmetry of within ±1.5mm. Some clinics use InBody body composition analysis to measure muscle mass ratio and differentiate between masseter hypertrophy.
[Clinical Insight] The incidence of mandibular nerve injury is reported as 12-18% with traditional saws and 3-5% with Piezo Surgery (Journal of Cranio-Maxillofacial Surgery, 2019).
| Test Item | Purpose | Normal Range/Criteria |
|---|---|---|
| CBCT Slice Thickness | Precise identification of nerve/blood vessel location | 0.4-0.625mm |
| Frontal Cephalo | Quantification of asymmetry | Midline deviation ≤2 degrees |
| InBody Muscle Mass | Differentiation of masseter hypertrophy | Facial muscle ratio 18-22% |
| 3D VSP Simulation | Pre-operative planning of osteotomy amount | Error margin ±1mm |
- Average CBCT scan time: 40-90 seconds
- Average VSP software analysis time: 2-3 hours
Step 2: Surgical Design — Osteotomy Line Planning and Fixation Selection
For square jaw osteotomy, a posterior resection of 15-22mm from the mandibular angle is standard, with simultaneous detachment of the masseter muscle attachment. The Long Curve osteotomy method connects the mandibular angle to the chin in a smooth curve to prevent secondary angle formation, with an average osteotomy line length of 7-9cm. Cheekbone reduction involves three methods: Type I (anterior osteotomy), L-shaped (lateral rotation), and T-shaped (superior repositioning), with the zygomatic arch typically moved posteriorly by 5-8mm.
Fixation after osteotomy uses Titanium Miniplates (0.5-1.0mm thickness) and Micro-screws (1.5-2.0mm diameter). Wire fixation, used until the early 2000s, is now rarely employed. Bioabsorbable plates (PLA/PLLA material) naturally degrade within 12-18 months but offer only 60% of the initial fixation strength compared to titanium. For chin T-osteotomy, one plate is used for 3-5mm advancement or setback, and two plates for movements exceeding 6mm.
[Key Point] Excessive osteotomy (over 25mm for square jaw) can lead to masticatory muscle weakness, reducing chewing force by an average of 32% compared to pre-surgery, and increasing temporomandibular joint load long-term.
- Titanium plate removal rate: 15-20% (for aesthetic reasons)
- Average PLA plate complete absorption period: 14 months
Step 3: General Anesthesia and Surgery — Real-time Monitoring
General anesthesia for contour surgery is induced with Propofol 2-2.5mg/kg and Remifentanil 0.1-0.3μg/kg/min. Nasal intubation is performed for airway management. To minimize intraoperative bleeding, 1g of Tranexamic acid is administered intravenously, reducing average blood loss from 350ml to 220ml.
Access is gained through intraoral incisions (square jaw, cheekbones) or extraoral incisions (part of the chin). Piezo Surgery equipment uses ultrasonic frequencies of 25-29kHz to selectively cut bone tissue, minimizing soft tissue damage. The average surgery time for simultaneous square jaw and cheekbone procedures is 2.5-3.5 hours, and for all three areas (square jaw, cheekbones, chin) it is 3.5-4 hours. A Nerve Monitoring System tracks the mandibular nerve's electrical signals in real-time during surgery, and osteotomy positions are adjusted if impedance increases by more than 30% from the baseline.
[Caution] Nasal intubation carries a risk of nasal septum injury, and nasal congestion and minor bleeding may occur for 3-5 days post-surgery.
- Nerve injury rate with Piezo device: 3-5% vs. traditional saw: 12-18%
- Average anesthesia maintenance duration: 2.5-4 hours
Step 4: Recovery Room — Intensive Observation for the First 24 Hours
Immediately after surgery, patients are monitored in the recovery room for an average of 2-4 hours, observing blood pressure, oxygen saturation, and drainage volume. A Hemovac drain removes hematoma under negative pressure of 100-150mmHg and is removed if the 24-hour drainage volume is less than 50ml. Continuous cold compresses (15 minutes on, 15 minutes off) for 48 hours can reduce peak swelling by an average of 18%.
Pain management is provided via a Fentanyl PCA (Patient-Controlled Analgesia) pump, set at a basal infusion rate of 0.5-1.0ml/h plus patient-controlled boluses of 0.5ml (with a 15-minute lockout period). Intraoral incision sites are disinfected 4-6 times daily with 0.12% Chlorhexidine mouthwash, and absorbable Vicryl 4-0 sutures are used, dissolving naturally within two weeks.
| Recovery Stage | Duration | Key Management Items |
|---|---|---|
| Immediate Recovery | 0-4 hours | Drain monitoring, maintaining oxygen saturation above 95% |
| Acute Swelling Phase | 1-3 days | Cold compresses for 48 hours, head elevated at 30 degrees, NPO progressing to liquids |
| Early Recovery Phase | 4-7 days | Transition to warm compresses, drain removal, semi-liquid diet initiation |
| Subacute Phase | 2-4 weeks | 60% swelling reduction, soft solid foods, light exercise |
| Late Recovery Phase | 1-3 months | 80-90% swelling resolution, normal diet, bone fusion progress |
| Full Recovery Phase | 6-12 months | Complete bone fusion, final contour established |
- Swelling peak reduced by 142% → 117% with 48 hours of cold compresses
- Average PCA usage duration: 2-3 days
Step 5: One Week Post-Op — Swelling Management and Dietary Adjustments
Swelling peaks around days 3-4 post-surgery, with facial volume increasing by an average of 142% compared to pre-operative levels. Sleeping with the head elevated at over 30 degrees during this period improves venous return, shortening the duration of swelling by an average of 1.2 days. From 72 hours onwards, switching to warm compresses (40-42°C, 15 minutes, 4-6 times daily) promotes blood circulation.
Diet progresses from NPO on days 1-2, to liquids like rice porridge and grain powder on days 3-4, and then to semi-liquid foods such as tofu and steamed eggs on days 5-7. Chewing motions place mechanical stress on the osteotomy sites and are prohibited for at least two weeks. Adequate protein intake (60-80g per day) is essential for tissue regeneration. While one study suggests that taking 500mg of Bromelain three times daily can accelerate swelling reduction by an average of 22%, it is contraindicated for patients on anticoagulants.
[Nutrition] Insufficient protein can delay bone fusion. Calcium (1000mg/day) + Vitamin D (800-1000IU/day) supplementation is recommended.
- Peak swelling time: average 72-96 hours
- Swelling reduction rate in the first week: approximately 30-40%
Step 6: 1-3 Months — Bone Fusion and Nerve Recovery

Bone fusion at the osteotomy site begins around week 2, with initial callus formation by week 6. Complete bony union requires a minimum of 6 months. During this period, excessive chewing (hard foods, gum, dried squid) can cause diastasis of the osteotomy line, potentially requiring revision surgery if plates loosen.
Mandibular nerve injury results in reduced sensation (paresthesia) in the lower lip and chin area, which typically recovers naturally within 3-6 months. Nerve regeneration progresses at an average of 1mm per day, meaning a distance of 30mm from the osteotomy site to the mental foramen would take approximately 30 days to bridge. Methylcobalamin (Methycobal) taken three times daily at 1500μg has been reported to accelerate nerve recovery by an average of 18%. Swelling decreases to 60% at 1 month and 80-90% at 3 months, with the final contour established between 6-12 months.
- Minimum 6 months for complete bone fusion
- Nerve recovery rate within 6 months: 92-97%
Step 7: Long-Term Follow-up — Relapse Prevention and Plate Removal
The recurrence rate of masseter hypertrophy after contour surgery is approximately 12-18% over a 5-year follow-up, often linked to chewing habits (preferring one side, favoring hard foods). Re-injection of Botulinum toxin A (Botox, Dysport) at 50-100U (total for both sides) every 6 months can reduce the recurrence rate to below 5%.
The optimal time for Titanium plate removal is 12-18 months post-surgery, with a removal rate of about 15-20%. The removal procedure takes an average of 30-60 minutes and can be performed under local or twilight anesthesia. If not removed, potential issues include metal allergies (if nickel-containing), MRI artifacts, and cold sensitivity (feeling cold in winter), though most cases are asymptomatic.
[Follow-up] Even after plate removal, a subtle osteotomy line remains permanently and is visible on CT scans due to differences in bone density.
- Masseter hypertrophy recurrence rate over 5 years: 12-18%
- Recommended timing for plate removal: 12-18 months
Comparison of Osteotomy Fixation Materials
Titanium Miniplate [Standard]
- Thickness: 0.5-1.0mm
- Fixation strength: 100% baseline
- Removal rate: 15-20%
- Potential for MRI artifacts
Most widely used, with proven long-term stability.
Bioabsorbable Plate (PLA/PLLA) [Absorbable]
- Thickness: 1.0-1.5mm
- Fixation strength: 60% (initial)
- Complete absorption within 12-18 months
- No removal surgery required
Less initial fixation strength, unsuitable for extensive osteotomies.
Wire Fixation [Obsolete]
- Diameter: 0.4-0.6mm
- Fixation strength: 40%
- Removal rate: Nearly 100%
- Rarely used since the 2000s
A method rarely employed today.
Common Misconceptions
Misconception: Full recovery from contour surgery takes only 1 month.
Truth: While swelling reduces by about 60% by month 1, bone fusion requires at least 6 months, and the final contour is established at 12 months. Consuming hard foods or engaging in strenuous exercise within 3 months carries a risk of osteotomy line separation.
Misconception: Plates must always be removed.
Truth: Titanium plates are usually asymptomatic if left in place, and the removal rate is only 15-20%. Removal is considered only after 12-18 months for specific reasons such as metal allergies, planned MRI scans, or cold sensitivity.
What to Absolutely Avoid During Contour Surgery

- Taking anticoagulant medications or supplements (e.g., aspirin, omega-3, ginkgo biloba) for 2 weeks prior to surgery (average 2x increase in blood loss).
- Chewing motions for 2 weeks post-surgery (mechanical stress on osteotomy sites → plate loosening).
- Sleeping with the head lowered (reduced venous return → average 1.2-day increase in swelling duration).
- Saunas, hot tubs, or intense aerobic exercise within 3 months post-surgery (may interfere with bone fusion).
- Poor oral hygiene (risk of osteomyelitis if incision site becomes infected — incidence is 0.5-1%, but treatment is extremely difficult).
Frequently Asked Questions
Does having both square jaw and cheekbone reduction simultaneously double the recovery time?
While the surgery time is about 1.5 times longer than for a single area, the recovery period is not doubled. Swelling peaks and bone fusion occur concurrently, so the overall recovery time is approximately 1.2-1.3 times longer than for a single area. However, the initial post-operative swelling may be more pronounced.
Is Piezo Surgery truly safer than conventional saws?
Yes. Piezo devices use ultrasonic frequencies of 25-29kHz to selectively cut bone tissue without damaging soft tissues like nerves and blood vessels. Numerous studies show a reduction in mandibular nerve injury rates from 12-18% with traditional saws to 3-5% with Piezo devices (Journal of Cranio-Maxillofacial Surgery, 2019).
What happens if sensation doesn't return after surgery?
In cases of mandibular nerve injury, recovery is typically spontaneous within 3-6 months, with a recovery rate of 92-97%. Nerve regeneration progresses at an average of 1mm per day, so the recovery time depends on the distance between the osteotomy site and the mental foramen. Nerve tonics like Methylcobalamin can aid recovery. If sensation remains absent after 6 months, nerve reconstruction may be considered.
Doesn't more bone resection lead to better results?
No. Excessive resection of the square jaw (over 25mm) can weaken the masticatory muscles, reducing chewing force by an average of 32%, and may lead to secondary angle formation and accelerated aging (sagging jawline). Similarly, moving the cheekbones more than 8mm increases the risk of midface hollowing and the appearance of "Indian wrinkles." Adhering to optimal ranges (15-22mm for square jaw, 5-8mm for cheekbones) leads to higher long-term satisfaction.
What happens if I eat hard foods before bone fusion is complete?
Excessive chewing force during the early stages of bone fusion (weeks 2-6) can cause diastasis (separation) of the osteotomy line, potentially requiring revision surgery if the plates loosen. While soft solid foods are permissible after 6 weeks when callus formation begins, tough foods (dried squid, jerky) and hard foods (nuts, candies) should be avoided for at least 3 months.
Can asymmetry recur after surgery?
Yes. The recurrence rate due to masseter hypertrophy is 12-18% over a 5-year follow-up, often related to unilateral chewing habits. Re-injection of Botulinum toxin A (50-100U) every 6 months can reduce the recurrence rate to below 5%. Additionally, asymmetry due to bone resorption or plate loosening occurs in 1-2% of cases, making follow-up CT scans at 1, 3, and 5 years recommended.
This content is for informational purposes only and does not substitute medical advice. Always consult with a specialist before undergoing any procedure.