Laser Toning Principles and 7 Types, How to Choose by Skin Type | K-Dia
Skincare
Laser Toning Principles and 7 Types, How to Choose by Skin Type
K-Dia Editor· Editor2026.05.2979
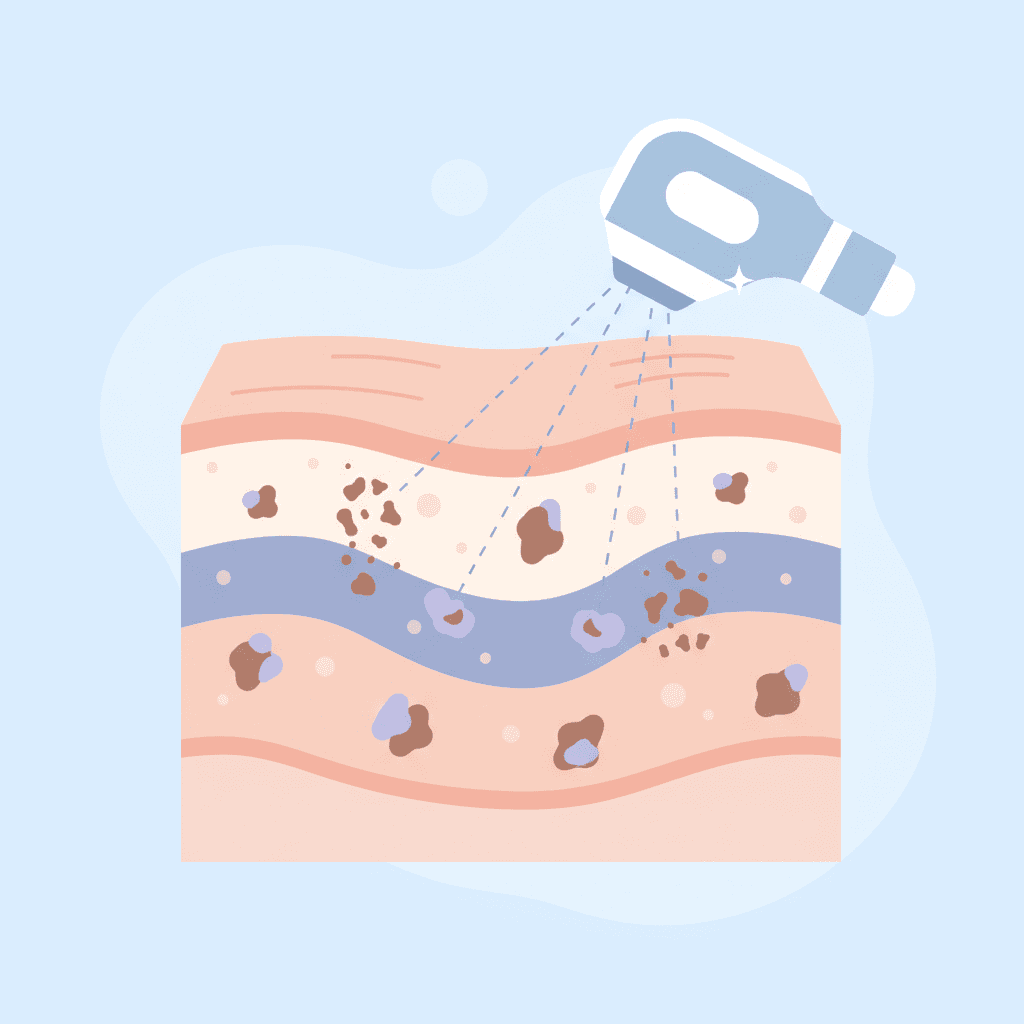
Laser toning removes pigmentation through the selective photothermal decomposition of melanin, with wavelength, pulse width, and energy density determining the results. Nd:YAG 1064nm targets melanin in the dermal layer, while 532nm targets epidermal blemishes, resulting in a three-fold difference in depth of action. Picosecond lasers reduce thermal damage by 90% through photoacoustic effects, making them suitable for Korean skin, which is at high risk for hyperpigmentation.
Analysis of Action Mechanisms by Wavelength
Wavelength 1064nm vs 532nm: 3x Difference in Penetration Depth
6-Step Low-Power Protocol Tailored for Korean Skin
One of the Most Frequently Asked Questions in the Clinic
“Isn’t laser toning just shooting a weak laser?” This single misconception ruins your choice of procedure.
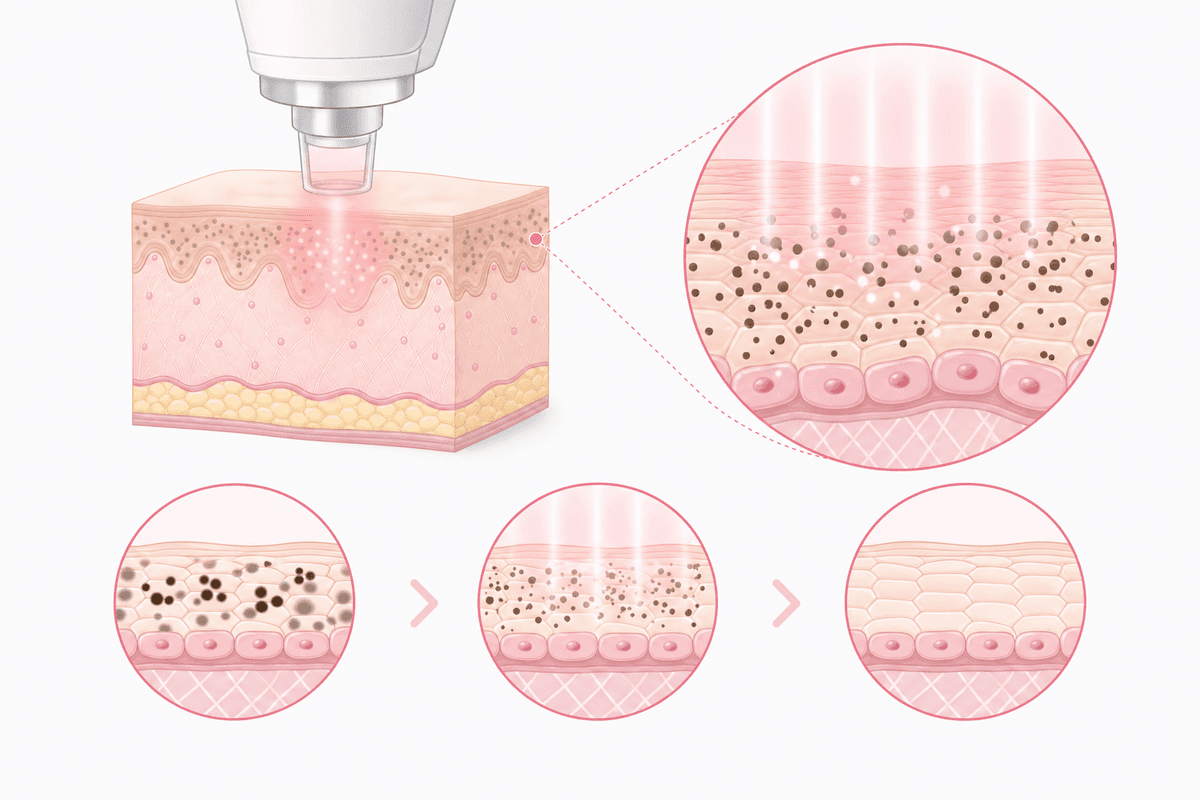
The key to laser toning is not output power, but **photothermal decomposition selectivity**. It irradiates specific wavelengths (1064nm, 532nm) that absorb only melanin at a dermal temperature of 45 degrees or lower to break down pigments without damaging surrounding tissues.
According to a 2013 study by the Korean Dermatological Association, even with the same wavelength, the pigment retention rate varies by 40% depending on the pulse width (5-10ns vs. 750ps).
The problem is that heat accumulates quickly due to the characteristics of Korean skin.
Because their melanin content is 2.5 times higher than that of Caucasians, the incidence of post-inflammatory hyperpigmentation (PIH) reaches 18-25%.
Therefore, rather than simply using low power, a three-step optimization process is required: **wavelength selection → pulse width setting → irradiation interval adjustment**.
Key Laser toning is not a 'weak laser' but a 'laser that controls selective photothermal decomposition'. Wavelength and pulse width determine 70% of the results.
Average melanin content in Koreans: 2.5 times that of Caucasians
Incidence of post-inflammatory hyperpigmentation: 18-25%
Difference in pigment retention rate with pulse width change: Up to 40%
Photothermal decomposition vs. Photoacoustic effects, differences in operating principles
Laser Toning — Photothermalysis vs. Photoacoustic Effect, Difference in Mechanism of Action
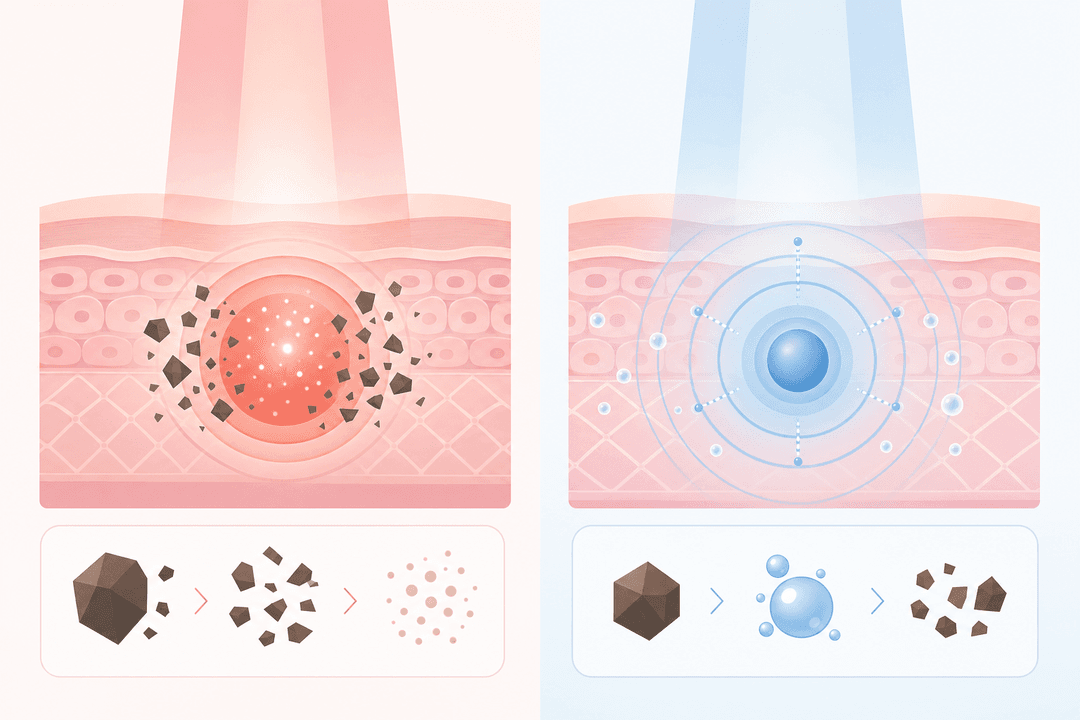
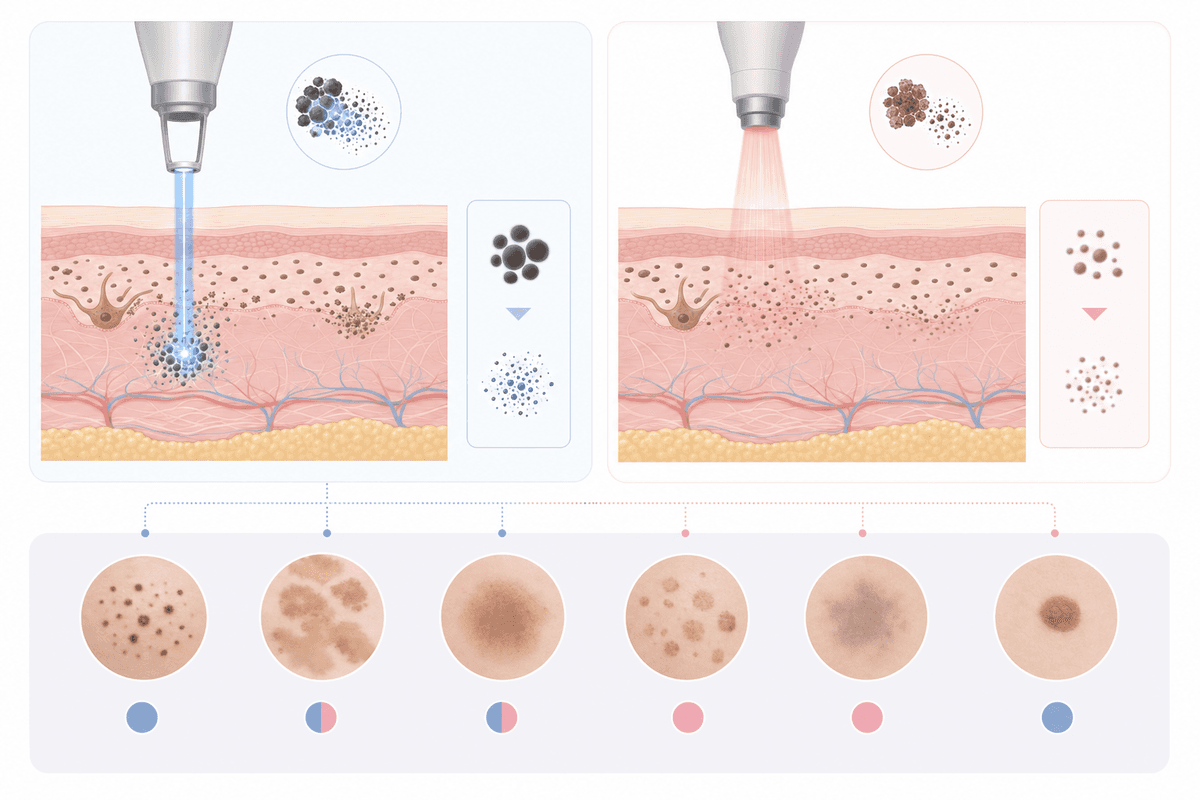
Nanosecond (ns) lasers use the **Photothermalysis** method. Light energy is converted into heat over 5-10ns, instantly raising the temperature of melanin to over 300 degrees to destroy it.
Nd:YAG 1064nm reaches the upper dermis (1.5-2mm) to target deep pigmentation and nevus of Ota. On the other hand, KTP 532nm is optimized for blemishes and freckles in the epidermal layer (0.3-0.5mm).
Picosecond (ps) lasers utilize the **Photoacoustic effect**. This is a method that physically breaks down melanin by generating only shock waves without thermal diffusion using pulses of 750 ps or less.
PicoSure (Cynosure), approved by the FDA in 2019, uses a 755nm alexandrite wavelength, and its melanin absorption is three times higher than that of Nd:YAG, resulting in superior decomposition efficiency even at the same energy level.
The key difference is thermal damage to surrounding tissues. While ns lasers raise epidermal temperature by 5-8 degrees due to a thermal diffusion time of 100-300 ns, ps lasers only raise it by 0.5-1 degree.
Clinical Picosecond lasers reduce thermal damage by 90%, resulting in a lower risk of PIH. It is given priority consideration in high-risk groups for pigmentation, such as patients with liver disease and long-term steroid users.
Classification
Nanosecond (ns)
Picosecond (ps)
Pulse Width
5-10ns
450-750ps
Mechanism of Action
Photothermal Decomposition
Photoacoustic Effect
Epidermal Temperature Elevation
5-8 degrees
0.5-1 degree
PIH Incidence
18-25%
8-12%
PicoSure 755nm: Melanin absorption 3 times higher than Nd:YAG
ns laser thermal diffusion time: 100-300ns
ps laser epidermal temperature rise: 0.5-1 degree
7 types by wavelength, different target depths
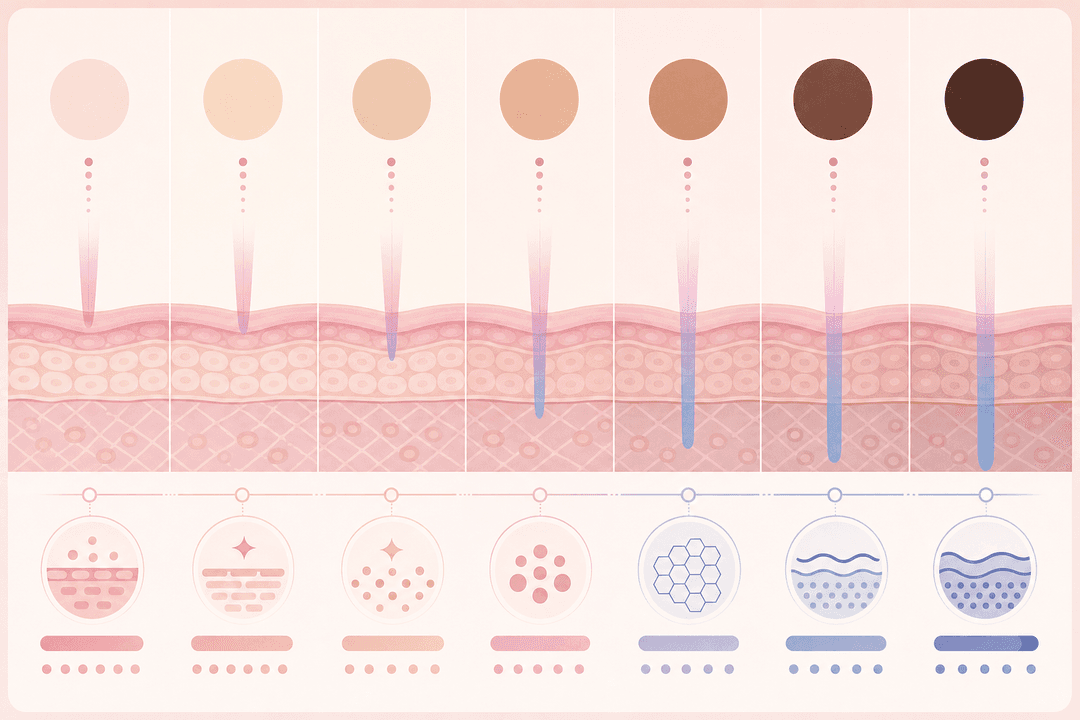
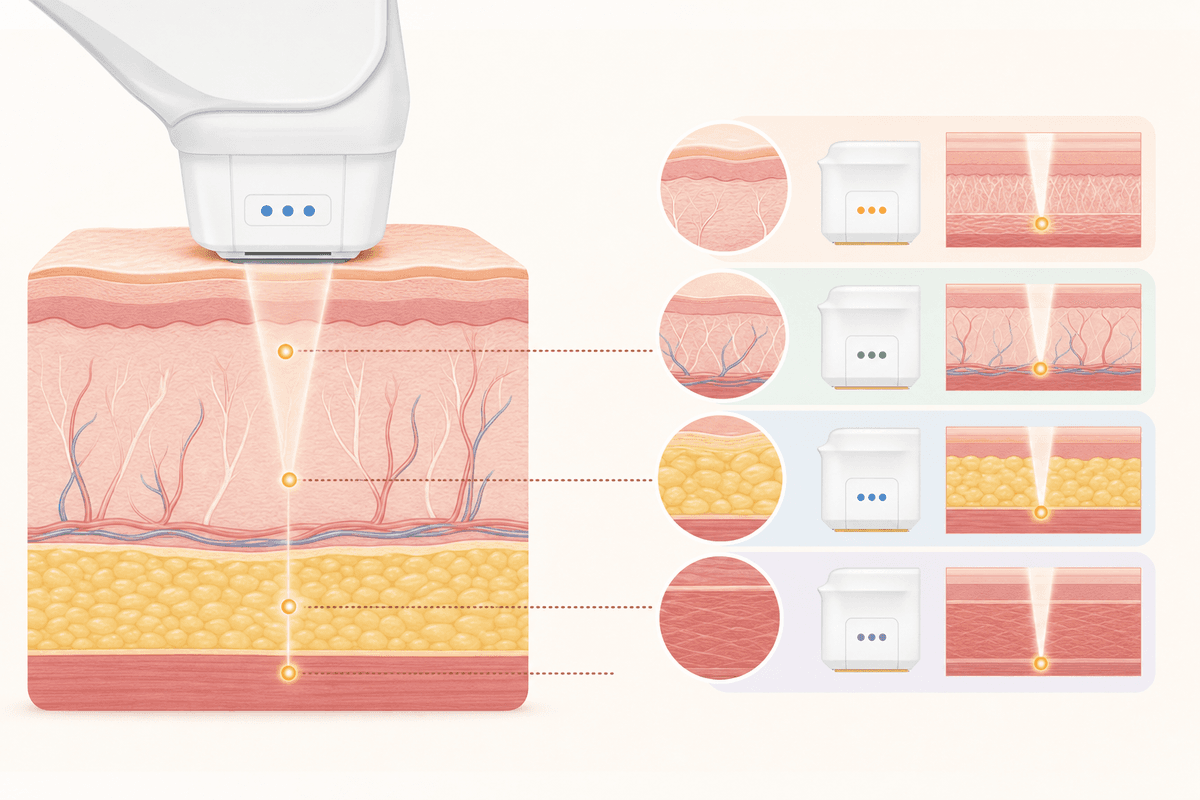
**1064nm Nd:YAG**: Reaches upper dermis (1.5-2mm). Used for removing deep melasma, nevus of Ota, and tattoos. Spectra XT (Lutronic) and RevLite SI (Cynosure) are representative examples.
**755nm Alexandrite**: High level of melanin absorption. Effective for pigments at the epidermal-dermal junction (0.8-1.2mm). PicoSure and PICOCARE have adopted this wavelength.
**532nm KTP**: Concentrated on the epidermal layer (0.3-0.5mm). Targets freckles, blemishes, and vascular lesions. Due to high hemoglobin absorption, it is also used in conjunction with treatment for red melasma.
**694nm Ruby**: Highest melanin selectivity, but poses a risk of burns on darker skin. Dedicated to blemishes on fair skin. Rarely used in Korea.
**Picosecond 585nm**: Vascular laser range. Improves red pigments and capillary dilation. It is equipped in the Discovery Pico Plus.
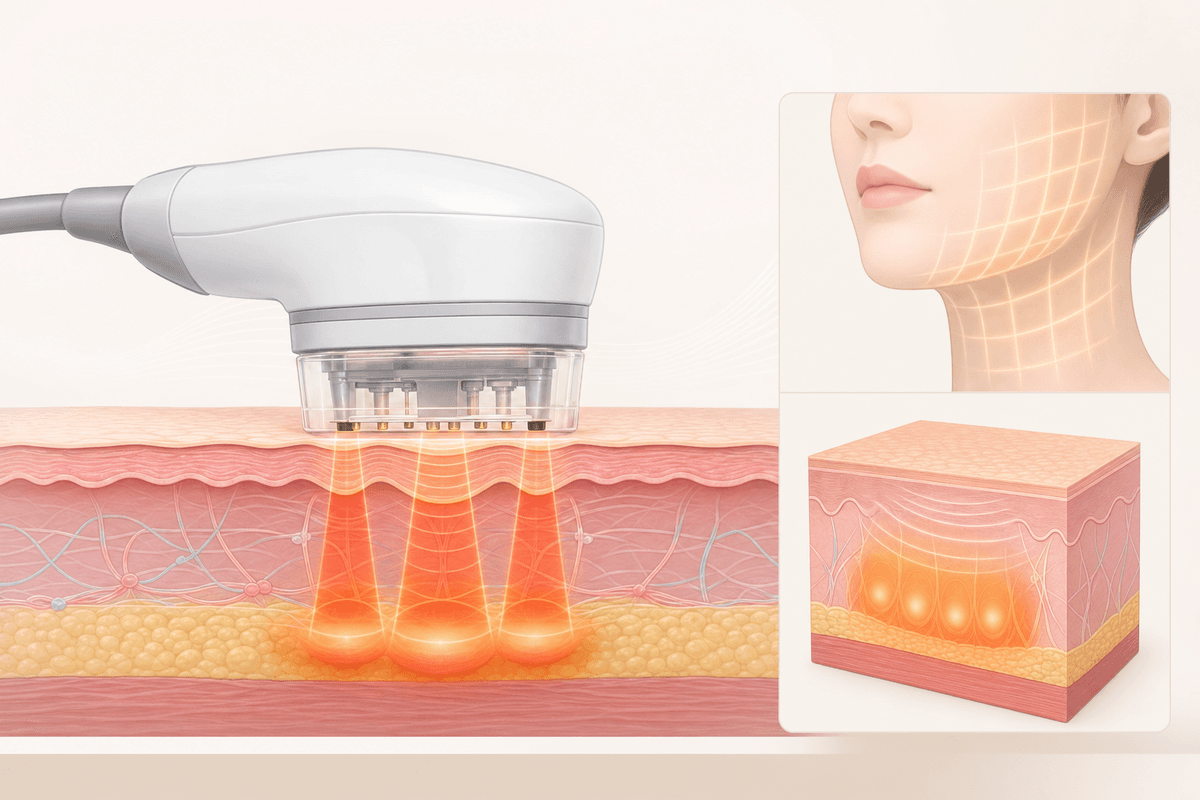
**1320nm Nd:YAG**: Collagen remodeling through thermal stimulation of the mid-dermal layer (3-4mm). Used in conjunction when the goal is to improve elasticity rather than pigmentation.
**650-1200nm IPL**: Broadband light. Weaker than laser toning, but capable of improving mild pigmentation and redness. Strictly speaking, it is not toning, but phototherapy.
1064nm penetration depth: 1.5-2mm (upper dermis)
755nm melanin absorption rate: 3 times compared to 1064nm
532nm hemoglobin absorption rate: 5 times compared to 1064nm
Selection method by skin type — Fitzpatrick classification criteria
Laser Toning — Selection Method by Skin Type — Fitzpatrick Classification Criteria
**Type I-II (Fair Skin)**: Low melanin content allows for all wavelengths. 694nm Ruby and 755nm Alexandrite are effective. However, if blood vessel projection is visible, 532nm is used in conjunction.
**Type III-IV (Average Korean)**: 1064nm Nd:YAG is the standard. 532nm should be used at a limited low energy level (2.0-2.5 J/cm²). Picosecond lasers are advantageous for securing a safety margin.
**Type V-VI (Dark Skin)**: Risk of burns with 755nm or lower. Use only 1064nm and increase the pulse width to 10ns or more to reduce heat diffusion.
The 2020 guidelines of the Korean Society of Dermatological Lasers recommend a test shot for Type IV or higher. This involves irradiating the area under the chin with 2-3 shots and checking the response for 48 hours.
If you have liver disease or are taking oral contraceptives, prioritize picosecond lasers regardless of skin type. This is because the rate at which heat accumulation causes hormonal pigmentation is 23% higher.
Caution: A test shot is mandatory for Type IV or higher. Checking the response for 48 hours before the actual procedure is the first step in preventing PIH.
Fitzpatrick Type
Recommended Wavelength
Precautions
I-II (Fair Skin)
694nm, 755nm, 1064nm
532nm in combination for vascular lesions
III-IV (Koreans)
1064nm, Pico 755nm
532nm is limited to low energy
V-VI (Dark Skin)
1064nm only
Pulse width of 10ns or more is mandatory
Recommendation for Type IV or higher testing: Korean Society of Laser Dermatology 2020
Incidence of heat-accumulated PIH in patients with liver disease: 23% high
Recommended pulse width for Type V-VI: 10ns or more
Energy density and spot size are not everything
Laser toning is typically performed in the range of 2.0-4.5J/cm². However, even with the same 3.0 J/cm², the penetration depth varies by 30% depending on the spot size (4mm vs. 8mm).
**Spot diameter 6-8mm**: Energy is dispersed and concentrated in the epidermal layer. Preferred when targeting blemishes and freckles.
**Spot diameter 4-5mm**: Energy density increases, reaching the dermis. Used for treating melasma and nevus of Ota.
Irradiation density is also a variable. Single pass controls the total energy amount with 20-30% overlap, while multi-pass controls it with 60-70% overlap.
According to 2018 clinical data from the Korean Dermatological Association, the multi-pass (3-session) protocol showed a 15% higher pigment removal rate compared to single pass, but the incidence of PIH also increased by 9%.
Therefore, it is common practice to check the skin response with a single pass for the initial treatment, and then switch to multi-pass starting from the 3rd or 4th session.
Tip: While the spot size and irradiation density are controlled by the medical staff, before the procedure, [whether] it is a single pass or multi-pass You can gauge the safety of the protocol just by asking.
Laser toning energy range: 2.0-4.5J/cm²
Difference in penetration depth with spot size change: Up to 30%
Multi-pass pigment removal rate: 15% higher compared to single pass
Multi-pass PIH incidence: 9% increase (Korean Dermatological Association 2018)
Suitable subjects, contraindications, and case-by-case judgment criteria
Laser Toning — Suitable Candidates and Contraindications, Case-by-Case Judgment Criteria
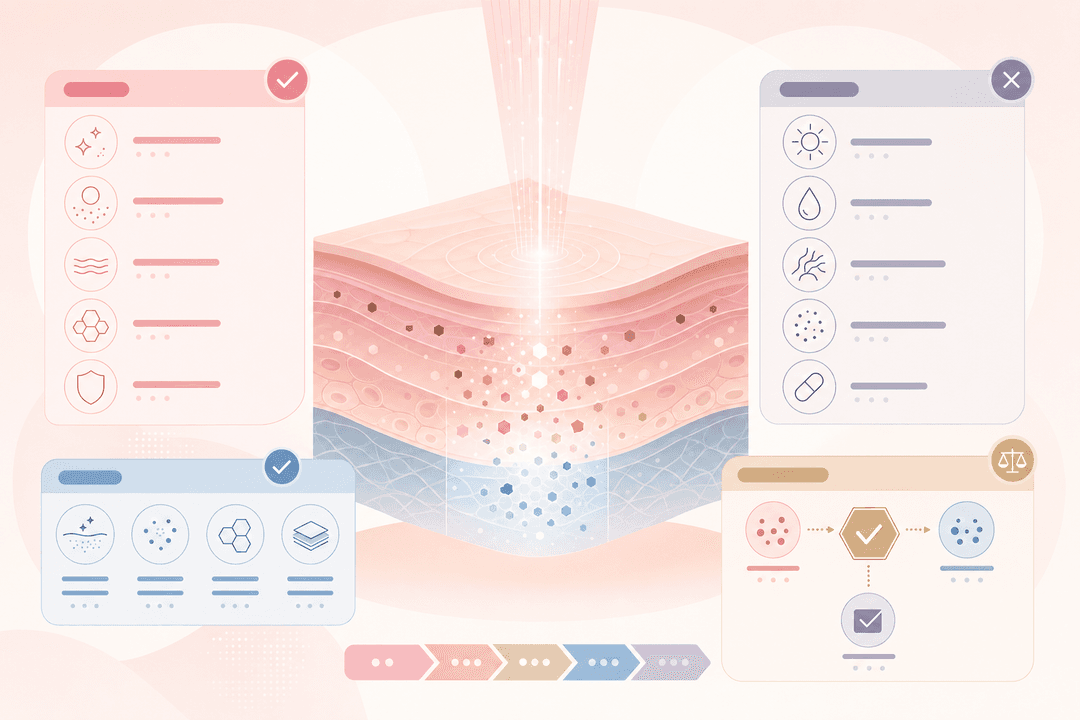
**Relative Contraindications**: History of photosensitivity, use of isotretinoin (Roaccutane) within the last 6 months, keloid predisposition, Pregnancy or breastfeeding, active herpes.
**Absolute contraindications**: Skin cancer at the treatment site, excessive UV exposure within the past month (immediately after an overseas vacation), active phase of autoimmune diseases (lupus, scleroderma).
Patients with liver disease have a 23% higher risk of hyperpigmentation due to reduced blood estrogen metabolism, so a picosecond laser or low-energy (2.0-2.5 J/cm²) protocol is applied.
If you are taking oral contraceptives or undergoing hormone therapy, thorough use of sunscreen (SPF 50+, PA++++) is essential for 2 weeks before and after the procedure. This is because hormones activate the melanin synthesis enzyme (tyrosinase) by 35%.
3-5 sessions are recommended for blemishes in your 20s, and 8-12 sessions for stubborn melasma in your 40s. This is because skin thickness and melanin distribution vary by age.
Caution
Laser toning is contraindicated if you are taking Roaccutane or have stopped taking it less than 6 months ago. Reduced skin regenerative capacity increases the risk of scarring threefold.
Risk of hyperpigmentation in liver disease patients: 23% higher
Hormone tyrosinase activation: 35%
Minimum waiting time to discontinue Roaccutane: 6 months
Average number of treatments for 20s: 3-5 times
Resistant melasma in 40s: 8-12 times
Comparison of Major Laser Toning Equipment
Spectra XT (Lutronic) [Nd:YAG]
Wavelength: 1064nm/532nm Dual
Pulse Width: 5ns
Suitable for: Deep melasma, nevus of Ota
Domestic Market Share: Approx. 40%
Most Rich Clinical Data on Korean Skin
PicoSure (Cynosure) [Picosecond]
Wavelength: 755nm Alexandrite
Pulse Width: 550-750ps
Suitable for: Epidermal-Dermal Barrier Pigmentation, High-Risk PIH Groups
Shortened Treatment Time with Simultaneous Multi-Wavelength Irradiation
Common Misconceptions
Misconception Laser toning is safe as long as the output is lowered
Truth **Pulse width and irradiation interval** determine safety more than output (energy). Even with the same energy, heat diffusion differs tenfold between a pulse width of 5ns and 750ps, and when irradiation densities overlap by more than 60%, the incidence of PIH increases by 9% due to heat accumulation. The key is not simply low output, but the optimization of the three factors of wavelength, pulse width, and density.
Misconception Doing it strongly at once can reduce the number of sessions
Truth The principle of laser toning is 'repeated low-output irradiation'. While high-energy single irradiation has a high rate of melanin destruction, the incidence of post-inflammatory hyperpigmentation (PIH) increases by up to 25%. Repeating the procedure 5-10 times at intervals of 2-3 weeks is a protocol that maintains a pigment removal rate of 70-80% while minimizing PIH to 8-12%.
Absolutely Prohibited Actions Before and After Laser Toning Procedure
Stop using cosmetics containing exfoliating ingredients such as retinol, AHA, and BHA starting 2 weeks before the procedure (Thinning of the stratum corneum doubles the risk of burns)
Do not apply thick makeup or sunscreen on the day of the procedure (Effectiveness is reduced by 30% due to laser energy reflection)
Avoid saunas, heat yoga, and excessive drinking within 24 hours immediately after the procedure (Increased PIH risk by 15% due to elevated dermal temperature)
Reapplying sunscreen (SPF 50+, PA++++) every 2 hours for 2 weeks after the procedure is essential (Melanin regeneration Blocking)
Do not forcibly remove dead skin cells from the treatment area (uneven pigmentation may occur due to interference with epithelial regeneration)
Do not shorten the treatment interval to less than 2 weeks (risk of burns and scarring increases 3 times if the stratum corneum does not recover)
Frequently Asked Questions
Laser Toning vs. Pico Toning, which is better?
Pico Toning is a type of laser toning with a pulse width in picosecond (ps) units. Compared to nanosecond (ns) lasers, it reduces thermal damage by 90%, resulting in a lower risk of PIH, making it suitable for patients with liver disease or those taking steroids. However, the equipment price is 2-3 times higher, making the cost per session 20-30% more expensive. If your skin type is IV or lower and you have no history of PIH, the NS laser is sufficient.
How many sessions are needed to see results?
3-5 sessions are recommended for mild blemishes, and 8-12 sessions for stubborn melasma. Treatments are performed at intervals of 2-3 weeks, and visible pigment reduction is observed starting from the 3rd session. However, individual differences are significant, and additional follow-up treatments may be necessary depending on hormonal status and UV exposure.
When can I apply makeup after the procedure?
You can apply makeup starting from the evening of the same day, but it is recommended to wait 24 hours before using high-coverage products. For 6-12 hours immediately after the procedure, the dermal temperature is 3-5 degrees higher, and oil-rich cosmetics can cause heat accumulation, increasing the risk of PIH by 15%. Apply only a thin layer of moisturizer and sunscreen.
Is it true that melasma can get darker?
If post-inflammatory hyperpigmentation (PIH) occurs, it may temporarily appear darker. Although the incidence rate among Koreans is high at 18-25%, it can be reduced to 8-12% through the use of picosecond lasers, low-energy protocols, and thorough UV protection. PIH naturally disappears after 3-6 months, and recovery is faster when combined with whitening ointment.
Can I get the treatment in the summer?
It is possible, but UV management is tricky. For 2 weeks after the procedure, reapply sunscreen every 2 hours, and a hat or parasol is essential. If you are planning an overseas vacation, complete the procedure at least 4 weeks in advance, or start 2 weeks after returning home. Excessive exposure to UV rays increases the melanin regeneration rate by 35%, halving the effectiveness of the procedure.
Can I combine this with other procedures?
A 2-week interval is recommended for Botox and fillers, a 4-week interval for IPL, and an 8-week interval for fractional lasers. If an invasive procedure is performed before the stratum corneum has recovered following laser toning, the inflammatory response becomes excessive, increasing the risk of scarring threefold. You must consult with a specialist in advance regarding any combination of procedures.
This content is for informational purposes only and does not replace medical advice. You must consult with a specialist before the procedure.
Find the right clinic for you on K-Dia