4 Types of Laminates: Results Differ Based on a 0.3mm Difference in Tooth Reduction
- 0.3mm difference in laminate veneer reduction can impact your teeth's condition after 10 years.
- Ceramics for aesthetics, zirconia for strength — selection criteria vary by front tooth position.
- No-prep veneers aren't a one-size-fits-all solution — suitable candidates account for less than 30% of all cases.
Information as of July 2026
Custom Selection Criteria by Tooth Type
- 0.3~0.7mm difference in reduction amount
- Ceramic vs. Zirconia lifespan: 10 years vs. 15 years
- No-prep suitability rate below 30%
0.5mm vs. 0.8mm: Why Do Dental Clinics Differ?
For the same front teeth, Clinic A might say 'we only shave 0.3mm,' while Clinic B insists '0.7mm is necessary.' Few people realize that a 0.3mm difference in reduction can determine tooth health 10 years later.
Laminates are a procedure where a thin layer of tooth surface is shaved off, and then a ceramic or zirconia shell is bonded. Reduction amounts are broadly categorized into four protocols: No-prep (0-0.3mm), Minimal-prep (0.3-0.5mm), Conventional-prep (0.5-0.7mm), and Full-prep (0.7-1.0mm).
The 2021 guidelines from the American Academy of Cosmetic Dentistry (AACD) recommend minimal prep as the basic standard, reporting that limiting the reduction to 0.5mm or less has a greater than 95% probability of staying within the enamel (the hard outer layer of the tooth).
Key Point The average enamel thickness is 0.7-1.0mm, but this varies significantly among individuals. If the enamel is breached and the dentin (the sensitive layer beneath the enamel) is reached, the risk of sensitivity increases more than threefold.
Reduction Amount and Suitable Candidates by Laminate Type
No-prep laminates involve virtually no tooth shaving (0-0.3mm) or just roughening the surface. Lumineers by Ultradent, Italy, are a prime example. They use ultra-thin ceramic shells, 0.2-0.3mm thick, bonded with minimal reduction.
However, they are suitable for less than 30% of all candidates. According to a 2019 clinical study by the Korean Academy of Prosthodontics, no-prep laminates showed a 5-year survival rate of over 90% only in cases with straight teeth, mild discoloration, and no protruding front teeth. If teeth are inwardly positioned or severely discolored, the shells can appear unnaturally thick, and the reduced bonding area increases the risk of detachment.
Minimal-prep laminates involve reducing 0.3-0.5mm. This allows for minimal shaving within the enamel layer, reducing tooth damage while ensuring adhesion and aesthetics. IPS e.max Press ceramic from Ivoclar Vivadent, USA, is commonly used, and over 70% of domestic dental clinics adopt this as their basic protocol.
Conventional prep involves 0.5-0.7mm reduction and is chosen for correcting severe discoloration, protrusion, or misalignment. Increased reduction carries a risk of exposing dentin, but it allows for thicker shells to mask color and alter shape. Full prep shaves up to 0.7-1.0mm, approaching the scope of a crown, and is applied to discolored teeth after root canal treatment or in cases of severe fractures.
| Protocol | Reduction Amount | Suitable Candidates | 5-Year Survival Rate |
|---|---|---|---|
| No-prep | 0-0.3mm | Straight teeth, mild discoloration | 90% (Conditional) |
| Minimal-prep | 0.3-0.5mm | General aesthetic improvement | Over 95% |
| Conventional-prep | 0.5-0.7mm | Severe discoloration, protrusion | 93% |
| Full-prep | 0.7-1.0mm | After root canal, fracture | 90% |
Survival rates are based on the 2021 AACD meta-analysis and may vary depending on individual oral conditions and care.
- Average enamel thickness 0.7-1.0mm — exceeding this risks dentin exposure
- No-prep suitability rate below 30% — limited to cases with straight teeth and mild discoloration
- Minimal-prep 5-year survival rate over 95% — standard protocol in Korea
- Full-prep is an alternative to crowns — applied to discolored teeth after root canal treatment
True/False Quiz
No-prep laminates involve minimal tooth reduction and are safe for everyone.
Check Answer
X No-prep is only suitable for less than 30% of candidates with straight teeth and mild discoloration. If enamel is thin or there's severe discoloration/protrusion, the shells appear thick, and the detachment rate increases more than threefold.
Ceramic vs. Zirconia: Material Determines Lifespan
Ceramic laminates offer high translucency, best replicating the light transmission of natural teeth. IPS e.max Press (lithium disilicate ceramic) is a representative example, with a flexural strength of 400MPa, suitable for front teeth. A 2020 study in the Journal of Prosthetic Dentistry reported a 10-year survival rate of 92.3% for ceramic laminates.
However, their drawback is strength. They are not suitable for molars or areas with strong occlusal forces, and there's a risk of fracture with severe bruxism. The cost ranges from 800,000 to 1.2 million KRW per tooth.
Zirconia laminates have a flexural strength of 900-1,200MPa, more than double that of ceramic. Examples include Lava Esthetic by 3M, Germany, and IPS e.max ZirCAD by Ivoclar, Switzerland. With a 15-year survival rate of over 96%, they are used for cases requiring long-term durability or on adjacent areas of canines and molars.
However, their lower translucency means ceramic is often preferred for the two central incisors for a more natural look. The price is 20-30% higher than ceramic, ranging from 1 million to 1.5 million KRW per tooth.
Clinical Insight Over 60% of dental clinics in Korea use a combination of ceramic for the two central incisors and zirconia for the four lateral incisors. This strategy balances aesthetics and strength.
- Ceramic flexural strength 400MPa, Zirconia 900-1,200MPa
- Ceramic 10-year survival rate 92.3%, Zirconia 15-year survival rate over 96%
- Combination of ceramic for central incisors and zirconia for lateral incisors used by over 60%
- Price difference 20-30% — Zirconia is more expensive but offers superior long-term durability
Selection Criteria by Tooth Position — Central Incisors vs. Lateral Incisors Differ
The two central incisors are most visible when smiling, making aesthetics the top priority. Ceramics like IPS e.max Press are standard, with minimal prep (0.3-0.5mm) performed within the enamel layer. For severe discoloration, conventional prep (0.5-0.7mm) is used to achieve sufficient thickness for color masking.
The four adjacent front teeth (lateral incisors, canines) experience greater occlusal forces and more contact with food than central incisors. Zirconia is used to enhance durability, or if ceramic is used, a thickness of 0.5mm or more is ensured. Canines, in particular, are prone to wear from bruxism, leading to over 80% of applications using zirconia.
The lower front teeth have thinner enamel (average 0.5-0.7mm) and greater occlusal pressure than the upper front teeth. No-prep carries a higher risk of detachment, so minimal prep or more is recommended. A 2020 report from the Korean Academy of Prosthodontics showed a 3-year detachment rate of 15% for lower front teeth no-prep laminates, three times higher than for upper front teeth (5%).
| Tooth Position | Recommended Material | Recommended Reduction Amount | Key Considerations |
|---|---|---|---|
| Central Incisors (2 front teeth) | Ceramic | 0.3-0.5mm | Aesthetics paramount |
| Lateral Incisors (2 adjacent front teeth) | Ceramic or Zirconia | 0.5-0.7mm | Consider occlusal forces |
| Canines | Zirconia | 0.5-0.7mm | Prepare for bruxism wear |
| Lower Front Teeth | Zirconia | 0.3-0.5mm | Thin enamel, risk of detachment |
Individual customization is necessary based on tooth condition and occlusion; the above are general recommendations.
Bruxism and Occlusal Pressure: Hidden Variables
Nighttime bruxism (teeth grinding) increases the risk of laminate fracture by more than fourfold. A 2018 study in the Journal of Esthetic and Restorative Dentistry found that the 5-year laminate fracture rate in bruxism patients was 18%, significantly higher than the 4% in non-bruxism patients.
Occlusal form is also crucial. If the front teeth meet edge-to-edge or if the lower front teeth push against the upper front teeth (underbite), crowns are safer than laminates. Even with minimal prep, thin shells cannot withstand the pressure.
Age and enamel thickness are also variables. In their 20s, enamel is thicker (average 1.0mm) with better regenerative capacity, making minimal prep sufficient. However, for individuals over 50, enamel wears down to an average of 0.6mm, so attempting no-prep carries a high risk of exposing dentin.
Caution If you suffer from bruxism, wearing a night guard is essential. Even after laminate placement, sleeping without a guard increases the fracture probability to over 20% within two years.
- 5-year fracture rate in bruxism patients 18% vs. non-bruxism patients 4% — a fourfold difference
- Crowns recommended over laminates for edge-to-edge occlusion
- Average enamel thickness in 20s is 1.0mm, in 50s is 0.6mm — reduction amount needs adjustment by age
- Risk of fracture within 2 years exceeds 20% without a night guard
Key Takeaways — Reduction Amount and Material Vary by Tooth
Laminates are a combination of 'how much is shaved' and 'what is bonded.' A 0.3mm difference in reduction can determine whether you stay within the enamel or go beyond, and the choice of material dictates the outcome after 10 years.
The current clinical standard is to use ceramic for central incisors to achieve aesthetics, and zirconia for lateral incisors and canines to ensure strength. For those with bruxism or high occlusal pressure, night guards and regular check-ups, rather than just the material, determine the survival rate.
- Request enamel thickness measurement during consultation — can be checked with CT or panoramic X-rays
- Always disclose if you have bruxism — to plan for a night guard
- Consider combining ceramic for central incisors with zirconia for lateral incisors and canines
- Early detection of detachment/fracture through regular check-ups at 6 months, 1 year, and 2 years post-procedure
Ceramic vs. Zirconia Material Comparison
Ceramic (IPS e.max Press) [Aesthetics First]
- Flexural Strength: 400MPa
- 10-Year Survival Rate: 92.3%
- High Translucency — Similar to natural teeth
- Price: 800,000-1,200,000 KRW/piece
Optimal for the two central incisors
Zirconia (IPS e.max ZirCAD) [Durability First]
- Flexural Strength: 900-1,200MPa
- 15-Year Survival Rate: Over 96%
- Low Translucency — Slightly opaque
- Price: 1,000,000-1,500,000 KRW/piece
Suitable for canines and bruxism patients
Combination Strategy [Balance]
- Ceramic for central incisors + Zirconia for lateral incisors/canines
- Achieves both aesthetics and strength
- Adopted by over 60% of Korean dental clinics
- Total cost: 5-7 million KRW (for 6 front teeth)
The most common choice
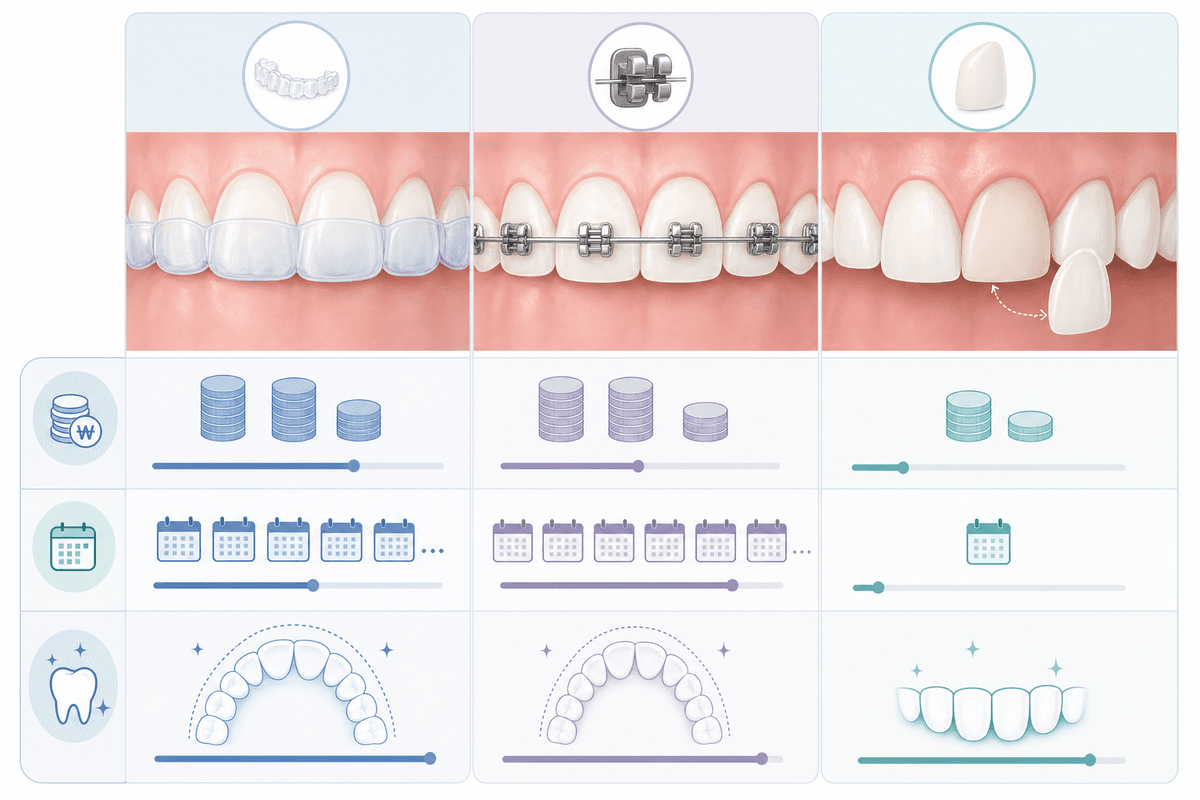
Which Laminate is Right for My Teeth?
If your teeth are straight with only minor discoloration
Minimal-prep ceramic (0.3-0.5mm)
Ensures over 95% 5-year survival rate with minimal reduction within enamel
If you want to correct severe discoloration, protrusion, or misalignment in one go
Conventional-prep zirconia (0.5-0.7mm)
Thicker shells correct color and shape simultaneously, with excellent durability
If you have bruxism or strong occlusal pressure
Zirconia + Night guard is essential
Minimizes fracture risk with flexural strength over 900MPa; guard increases 2-year survival rate from 80% to 95%
If you are over 50 or have thin enamel
Minimal-prep or more recommended; avoid no-prep
Average enamel thickness is 0.6mm, increasing dentin exposure risk threefold with no-prep
Common Misconceptions
Myth It's always best to avoid shaving teeth for laminates.
Truth No-prep is only suitable for less than 30% of candidates with straight teeth and mild discoloration. Minimal reduction within the enamel layer (0.3-0.5mm) is the standard that balances adhesion and aesthetics.
Myth Ceramic is always more beautiful than zirconia.
Truth While ceramic is more natural for the two central incisors, zirconia reduces fracture risk fourfold for canines and bruxism patients. Differentiating materials by position and occlusion is the current clinical standard.
Must-Knows Before Laminate Procedure
- Confirm enamel thickness measurement via CT or panoramic X-ray — avoid no-prep if less than 0.5mm
- Accurately disclose bruxism/occlusal form — hiding it increases fracture risk by over 20% within 2 years
- Specify material brand and reduction amount in the contract — to prevent post-procedure disputes
- Check if night guard fabrication cost is included — essential for bruxism patients
- Schedule regular check-ups at 6 months, 1 year, and 2 years post-procedure — early detection of detachment/fracture triples success rates
Frequently Asked Questions
How long do laminates last after the procedure?
Ceramics have a 10-year survival rate of 92.3%, and zirconia has a 15-year survival rate of over 96%. However, this can vary twofold to threefold depending on bruxism, occlusal pressure, and night guard usage.
Will shaving my teeth too much cause sensitivity?
If reduction stays within the enamel layer (average 0.7-1.0mm), the incidence of sensitivity is less than 5%. If reduction exceeds 0.7mm and reaches the dentin, the incidence increases to over 15%, a threefold rise.
Ceramic vs. Zirconia, which should I choose?
The standard practice for over 60% of Korean dental clinics is to use ceramic for the two central incisors (high translucency) and zirconia for lateral incisors and canines (double the strength). If you have bruxism, full zirconia is recommended.
How should I care for my teeth after laminate placement?
Avoid biting hard foods (ice, nuts) with your front teeth, wear a night guard (if you have bruxism), and attend regular check-ups every six months. Adhering to these three points increases the 10-year survival rate from 90% to 97%.
Are there any side effects of laminates?
The most common side effects are detachment (cumulative 5-year rate of 5-8%) and fracture (18% in bruxism patients). Rarely, gum inflammation (2-3%) may occur during bonding, or sensitivity due to excessive reduction (15% if enamel is exceeded). Enamel thickness measurement and disclosure of bruxism before the procedure are essential.
Is there a price difference between no-prep and minimal-prep?
No-prep costs 700,000-1,000,000 KRW per piece, while minimal-prep costs 800,000-1,200,000 KRW, a 10-20% difference. However, since no-prep has limited suitability, minimal-prep can be more economical when considering the cost of re-treatment after detachment.
Lumi's Note
A 0.3mm difference in reduction can make a difference 10 years later, showing how crucial details are! The key isn't 'how little is shaved,' but 'is it shaved appropriately for my teeth?' Be sure to request enamel thickness measurement during your consultation, and feel free to visit again if you have any questions about procedures.
This content is for informational purposes only and does not substitute medical advice. Always consult with a specialist before undergoing any procedure.